{"title":"射频消融治疗复发性肝癌:局部肿瘤进展与肝内远处复发的10年预后","authors":"Huan-Ling Guo, Jia-Qian Yao, Xin Zheng, Tong-Yi Huang, Xiao-Er Zhang, Rui Zhang, Wen-Xin Wu, Xiao-Yan Xie, Ming Xu","doi":"10.1186/s13244-025-02080-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To compare the long-term outcome of radiofrequency ablation (RFA) for local tumor progression (LTP) vs intrahepatic distant recurrence (IDR) in recurrent hepatocellular carcinoma (rHCC), including cases with repeated LTP.</p><p><strong>Materials and methods: </strong>From 2010 to 2022, 1326 rHCC patients treated with curative-intent RFA were identified. Propensity score matching (PSM) was used to balance the bias between the LTP group and the IDR group. Overall survival (OS) and progression-free survival (PFS), were compared between groups using log-rank tests and Cox proportional hazards models.</p><p><strong>Results: </strong>A total of 584 patients were finally enrolled (125 LTPs, 459 IDRs), with a median follow-up of 5.8 years. After PSM, 218 patients (109 patients in each group) were selected. The median OS was comparable between LTP and IDR (70.3 months vs 93.1 months, p = 0.974). However, PFS was significantly worse in the LTP group (13.8 months vs 20.9 months, p = 0.028). LTP incidence was higher in the LTP group (42.2% vs 12.8%, p < 0.001). Multiple recurrences, early recurrence (≤ 1 year), and ≥ 3 LTP episodes were independent risk factors for OS. The median OS decreased with increasing LTP episodes (0: 99.3 months; 1: 86.9 months; 2: 88.9 months; ≥ 3: 44.9 months, p = 0.031).</p><p><strong>Conclusions: </strong>RFA demonstrated effective control of LTP in rHCC, with comparable OS but worse PFS compared with IDR, primarily due to the higher risk of LTP. RFA may not be the first choice for those with ≥ 3 LTP episodes.</p><p><strong>Critical relevance statement: </strong>LTP of hepatocellular carcinoma shows higher recurrence than IDR after RFA, requiring close follow-up. Three or more repeat LTPs significantly worsen prognosis, suggesting the need for alternative treatment strategies.</p><p><strong>Key points: </strong>Long-term outcomes of RFA for LTP vs IDR of hepatocellular carcinoma remain unclear. LTP has worse PFS; ≥ 3 repeat LTP significantly worsens OS. LTP tends to recur after RFA, requiring close follow-up; ≥ 3 repeat LTPs need alternative local treatment.</p>","PeriodicalId":13639,"journal":{"name":"Insights into Imaging","volume":"16 1","pages":"191"},"PeriodicalIF":4.5000,"publicationDate":"2025-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12440844/pdf/","citationCount":"0","resultStr":"{\"title\":\"Radiofrequency ablation for recurrent hepatocellular carcinoma: 10-year outcomes of local tumor progression vs intrahepatic distant recurrence.\",\"authors\":\"Huan-Ling Guo, Jia-Qian Yao, Xin Zheng, Tong-Yi Huang, Xiao-Er Zhang, Rui Zhang, Wen-Xin Wu, Xiao-Yan Xie, Ming Xu\",\"doi\":\"10.1186/s13244-025-02080-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To compare the long-term outcome of radiofrequency ablation (RFA) for local tumor progression (LTP) vs intrahepatic distant recurrence (IDR) in recurrent hepatocellular carcinoma (rHCC), including cases with repeated LTP.</p><p><strong>Materials and methods: </strong>From 2010 to 2022, 1326 rHCC patients treated with curative-intent RFA were identified. Propensity score matching (PSM) was used to balance the bias between the LTP group and the IDR group. Overall survival (OS) and progression-free survival (PFS), were compared between groups using log-rank tests and Cox proportional hazards models.</p><p><strong>Results: </strong>A total of 584 patients were finally enrolled (125 LTPs, 459 IDRs), with a median follow-up of 5.8 years. After PSM, 218 patients (109 patients in each group) were selected. The median OS was comparable between LTP and IDR (70.3 months vs 93.1 months, p = 0.974). However, PFS was significantly worse in the LTP group (13.8 months vs 20.9 months, p = 0.028). LTP incidence was higher in the LTP group (42.2% vs 12.8%, p < 0.001). Multiple recurrences, early recurrence (≤ 1 year), and ≥ 3 LTP episodes were independent risk factors for OS. The median OS decreased with increasing LTP episodes (0: 99.3 months; 1: 86.9 months; 2: 88.9 months; ≥ 3: 44.9 months, p = 0.031).</p><p><strong>Conclusions: </strong>RFA demonstrated effective control of LTP in rHCC, with comparable OS but worse PFS compared with IDR, primarily due to the higher risk of LTP. RFA may not be the first choice for those with ≥ 3 LTP episodes.</p><p><strong>Critical relevance statement: </strong>LTP of hepatocellular carcinoma shows higher recurrence than IDR after RFA, requiring close follow-up. Three or more repeat LTPs significantly worsen prognosis, suggesting the need for alternative treatment strategies.</p><p><strong>Key points: </strong>Long-term outcomes of RFA for LTP vs IDR of hepatocellular carcinoma remain unclear. LTP has worse PFS; ≥ 3 repeat LTP significantly worsens OS. LTP tends to recur after RFA, requiring close follow-up; ≥ 3 repeat LTPs need alternative local treatment.</p>\",\"PeriodicalId\":13639,\"journal\":{\"name\":\"Insights into Imaging\",\"volume\":\"16 1\",\"pages\":\"191\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2025-09-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12440844/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Insights into Imaging\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13244-025-02080-9\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Insights into Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13244-025-02080-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
摘要
目的:比较射频消融(RFA)治疗复发性肝细胞癌(rHCC)局部肿瘤进展(LTP)与肝内远处复发(IDR)的长期预后,包括反复LTP的病例。材料和方法:2010年至2022年,1326例rHCC患者接受治疗意图RFA治疗。使用倾向评分匹配(PSM)来平衡LTP组和IDR组之间的偏倚。采用log-rank检验和Cox比例风险模型比较两组间的总生存期(OS)和无进展生存期(PFS)。结果:最终共纳入584例患者(125例ltp, 459例idr),中位随访时间为5.8年。经PSM后,218例患者(每组109例)入选。LTP和IDR的中位OS具有可比性(70.3个月vs 93.1个月,p = 0.974)。然而,LTP组的PFS明显更差(13.8个月vs 20.9个月,p = 0.028)。LTP组的LTP发生率更高(42.2% vs 12.8%)。结论:RFA有效控制了rHCC的LTP,与IDR相比,其OS相当,但PFS更差,主要是由于LTP的风险更高。对于LTP≥3次发作的患者,RFA可能不是首选。关键相关性声明:肝细胞癌LTP术后复发率高于IDR,需要密切随访。三次或三次以上重复ltp显著恶化预后,提示需要其他治疗策略。重点:RFA治疗肝细胞癌LTP与IDR的长期预后尚不清楚。LTP的PFS较差;≥3次重复LTP显著恶化OS。RFA后LTP容易复发,需要密切随访;≥3例重复ltp需要替代局部治疗。
Radiofrequency ablation for recurrent hepatocellular carcinoma: 10-year outcomes of local tumor progression vs intrahepatic distant recurrence.
Objectives: To compare the long-term outcome of radiofrequency ablation (RFA) for local tumor progression (LTP) vs intrahepatic distant recurrence (IDR) in recurrent hepatocellular carcinoma (rHCC), including cases with repeated LTP.
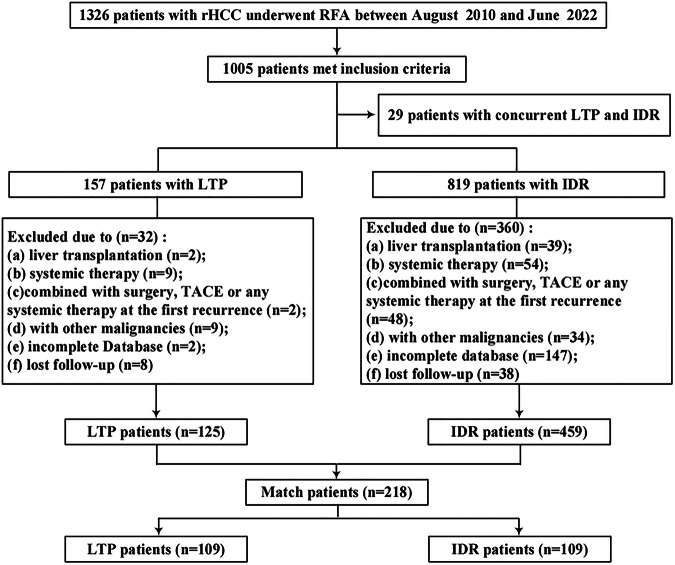
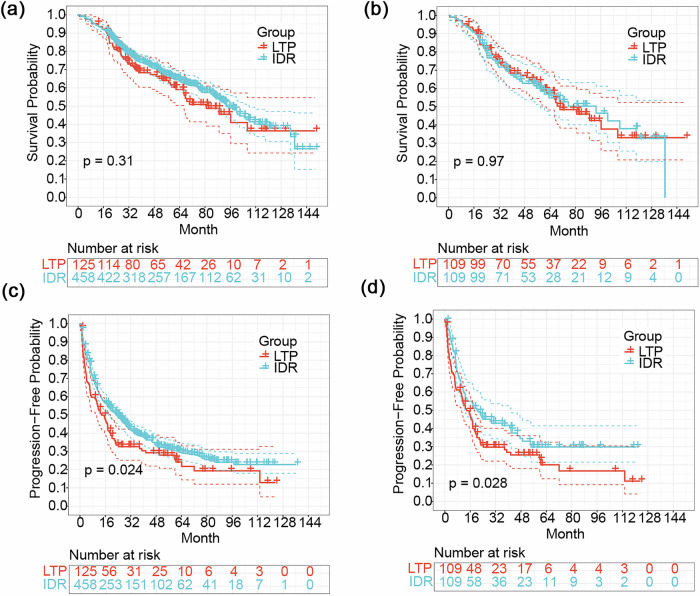
Materials and methods: From 2010 to 2022, 1326 rHCC patients treated with curative-intent RFA were identified. Propensity score matching (PSM) was used to balance the bias between the LTP group and the IDR group. Overall survival (OS) and progression-free survival (PFS), were compared between groups using log-rank tests and Cox proportional hazards models.
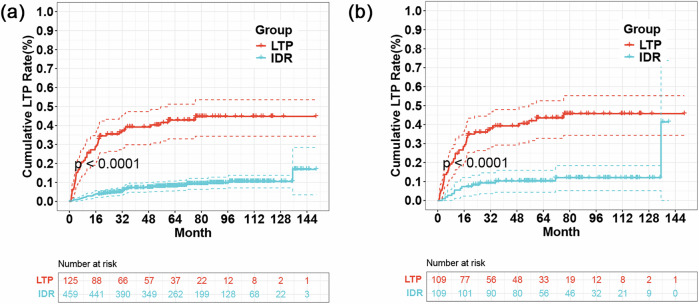
Results: A total of 584 patients were finally enrolled (125 LTPs, 459 IDRs), with a median follow-up of 5.8 years. After PSM, 218 patients (109 patients in each group) were selected. The median OS was comparable between LTP and IDR (70.3 months vs 93.1 months, p = 0.974). However, PFS was significantly worse in the LTP group (13.8 months vs 20.9 months, p = 0.028). LTP incidence was higher in the LTP group (42.2% vs 12.8%, p < 0.001). Multiple recurrences, early recurrence (≤ 1 year), and ≥ 3 LTP episodes were independent risk factors for OS. The median OS decreased with increasing LTP episodes (0: 99.3 months; 1: 86.9 months; 2: 88.9 months; ≥ 3: 44.9 months, p = 0.031).
Conclusions: RFA demonstrated effective control of LTP in rHCC, with comparable OS but worse PFS compared with IDR, primarily due to the higher risk of LTP. RFA may not be the first choice for those with ≥ 3 LTP episodes.
Critical relevance statement: LTP of hepatocellular carcinoma shows higher recurrence than IDR after RFA, requiring close follow-up. Three or more repeat LTPs significantly worsen prognosis, suggesting the need for alternative treatment strategies.
Key points: Long-term outcomes of RFA for LTP vs IDR of hepatocellular carcinoma remain unclear. LTP has worse PFS; ≥ 3 repeat LTP significantly worsens OS. LTP tends to recur after RFA, requiring close follow-up; ≥ 3 repeat LTPs need alternative local treatment.
期刊介绍:
Insights into Imaging (I³) is a peer-reviewed open access journal published under the brand SpringerOpen. All content published in the journal is freely available online to anyone, anywhere!
I³ continuously updates scientific knowledge and progress in best-practice standards in radiology through the publication of original articles and state-of-the-art reviews and opinions, along with recommendations and statements from the leading radiological societies in Europe.
Founded by the European Society of Radiology (ESR), I³ creates a platform for educational material, guidelines and recommendations, and a forum for topics of controversy.
A balanced combination of review articles, original papers, short communications from European radiological congresses and information on society matters makes I³ an indispensable source for current information in this field.
I³ is owned by the ESR, however authors retain copyright to their article according to the Creative Commons Attribution License (see Copyright and License Agreement). All articles can be read, redistributed and reused for free, as long as the author of the original work is cited properly.
The open access fees (article-processing charges) for this journal are kindly sponsored by ESR for all Members.
The journal went open access in 2012, which means that all articles published since then are freely available online.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


