{"title":"符合柏林定义的机械通气急性呼吸窘迫综合征患者弥漫性肺实质疾病的发生率","authors":"Yasuhiro Norisue, Ryohei Yamamoto, Hideki Yamakawa, Makoto Hibino, Tatsuya Nagai, Yutaro Fujimoto, Jun Kataoka, Kenji Ishii, Takashi Hongo, Daisuke Kasugai, Yudai Iwasaki, Masaaki Sakuraya, Goji Shimizu, Tomoyuki Masuyama, Shigeki Fujitani, Yasuharu Tokuda, Takashi Ogura","doi":"10.1183/23120541.01296-2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The simplicity of the diagnostic definition of acute respiratory distress syndrome (ARDS) has led to its diagnosis in patients with new-onset or exacerbation of diffuse parenchymal lung diseases (DPLDs). This study investigated the incidence of DPLDs in patients with acute hypoxic respiratory failure who met the Berlin definition.</p><p><strong>Methods: </strong>This Japan-based multicentre retrospective cohort study included patients on mechanical ventilation who met the Berlin definition. For all participants, diagnosis was made by pulmonology specialists in DPLD and thoracic radiology (blinded to clinical diagnoses) by reviewing an extensive database designed for DPLD diagnosis across 10 participating hospitals.</p><p><strong>Results: </strong>Of 13 612 patients admitted to the intensive care unit during the study period, 272 met the Berlin definition of ARDS and were included for analysis. All underwent at least one chest computed tomography scan; none underwent lung biopsy. Briefly, 182 were designated classic ARDS (67%), 69 non-IPF (idiopathic pulmonary fibrosis) DPLDs (25%) and 21 IPF (8%) by DPLD specialists. Of the 90 patients diagnosed with DPLD (IPF or non-IPF) by specialists, 35% were diagnosed with classic ARDS by intensivists at the end of the clinical course. Diagnostic classifications of classic ARDS and IPF by DPLD specialists were associated with time-to-death (adjusted hazard ratio (HR) 1.58 (95% CI 1.03-2.45), p=0.038, and adjusted HR 1.73 (95% CI 1.01-2.97), p=0.045, respectively) and in-hospital mortality (adjusted HR 1.54 (95% CI 1.06-2.23), p=0.022 for classic ARDS) <i>versus</i> non-IPF DPLDs; intensivist diagnostic classifications were not.</p><p><strong>Conclusion: </strong>Approximately one-third of patients within the Berlin definition were retrospectively diagnosed with new-onset or acutely exacerbated DPLD by specialists.</p>","PeriodicalId":11739,"journal":{"name":"ERJ Open Research","volume":"11 5","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12434489/pdf/","citationCount":"0","resultStr":"{\"title\":\"Incidence of diffuse parenchymal lung disease in patients meeting the Berlin definition of acute respiratory distress syndrome on mechanical ventilation.\",\"authors\":\"Yasuhiro Norisue, Ryohei Yamamoto, Hideki Yamakawa, Makoto Hibino, Tatsuya Nagai, Yutaro Fujimoto, Jun Kataoka, Kenji Ishii, Takashi Hongo, Daisuke Kasugai, Yudai Iwasaki, Masaaki Sakuraya, Goji Shimizu, Tomoyuki Masuyama, Shigeki Fujitani, Yasuharu Tokuda, Takashi Ogura\",\"doi\":\"10.1183/23120541.01296-2024\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The simplicity of the diagnostic definition of acute respiratory distress syndrome (ARDS) has led to its diagnosis in patients with new-onset or exacerbation of diffuse parenchymal lung diseases (DPLDs). This study investigated the incidence of DPLDs in patients with acute hypoxic respiratory failure who met the Berlin definition.</p><p><strong>Methods: </strong>This Japan-based multicentre retrospective cohort study included patients on mechanical ventilation who met the Berlin definition. For all participants, diagnosis was made by pulmonology specialists in DPLD and thoracic radiology (blinded to clinical diagnoses) by reviewing an extensive database designed for DPLD diagnosis across 10 participating hospitals.</p><p><strong>Results: </strong>Of 13 612 patients admitted to the intensive care unit during the study period, 272 met the Berlin definition of ARDS and were included for analysis. All underwent at least one chest computed tomography scan; none underwent lung biopsy. Briefly, 182 were designated classic ARDS (67%), 69 non-IPF (idiopathic pulmonary fibrosis) DPLDs (25%) and 21 IPF (8%) by DPLD specialists. Of the 90 patients diagnosed with DPLD (IPF or non-IPF) by specialists, 35% were diagnosed with classic ARDS by intensivists at the end of the clinical course. Diagnostic classifications of classic ARDS and IPF by DPLD specialists were associated with time-to-death (adjusted hazard ratio (HR) 1.58 (95% CI 1.03-2.45), p=0.038, and adjusted HR 1.73 (95% CI 1.01-2.97), p=0.045, respectively) and in-hospital mortality (adjusted HR 1.54 (95% CI 1.06-2.23), p=0.022 for classic ARDS) <i>versus</i> non-IPF DPLDs; intensivist diagnostic classifications were not.</p><p><strong>Conclusion: </strong>Approximately one-third of patients within the Berlin definition were retrospectively diagnosed with new-onset or acutely exacerbated DPLD by specialists.</p>\",\"PeriodicalId\":11739,\"journal\":{\"name\":\"ERJ Open Research\",\"volume\":\"11 5\",\"pages\":\"\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2025-09-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12434489/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ERJ Open Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1183/23120541.01296-2024\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ERJ Open Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1183/23120541.01296-2024","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
背景:急性呼吸窘迫综合征(acute respiratory distress syndrome, ARDS)诊断定义的简单性导致其在弥漫性肺实质疾病(DPLDs)新发或加重患者中得到诊断。本研究调查了符合柏林定义的急性缺氧呼吸衰竭患者DPLDs的发生率。方法:这项基于日本的多中心回顾性队列研究纳入了符合柏林定义的机械通气患者。所有参与者的诊断均由DPLD和胸部放射学专家(对临床诊断不知情)通过审查10家参与医院为DPLD诊断设计的广泛数据库做出。结果:在研究期间入住重症监护病房的13612例患者中,有272例符合ARDS的柏林定义,并被纳入分析。所有患者都接受了至少一次胸部计算机断层扫描;无一人接受肺活检。简而言之,182例为典型ARDS(67%), 69例为非IPF(特发性肺纤维化)DPLD(25%), 21例为IPF(8%)。在90例经专家诊断为DPLD (IPF或非IPF)的患者中,35%在临床过程结束时被重症监护医师诊断为典型ARDS。DPLD专家对经典ARDS和IPF的诊断分类与死亡时间(校正危险比(HR) 1.58 (95% CI 1.03-2.45), p=0.038,校正危险比(HR) 1.73 (95% CI 1.01-2.97), p=0.045)和院内死亡率(校正危险比1.54 (95% CI 1.06-2.23), p=0.022)与非IPF DPLD相关;强化诊断分类没有。结论:大约三分之一符合柏林定义的患者被专家回顾性诊断为新发或急性加重的DPLD。
Incidence of diffuse parenchymal lung disease in patients meeting the Berlin definition of acute respiratory distress syndrome on mechanical ventilation.
Background: The simplicity of the diagnostic definition of acute respiratory distress syndrome (ARDS) has led to its diagnosis in patients with new-onset or exacerbation of diffuse parenchymal lung diseases (DPLDs). This study investigated the incidence of DPLDs in patients with acute hypoxic respiratory failure who met the Berlin definition.
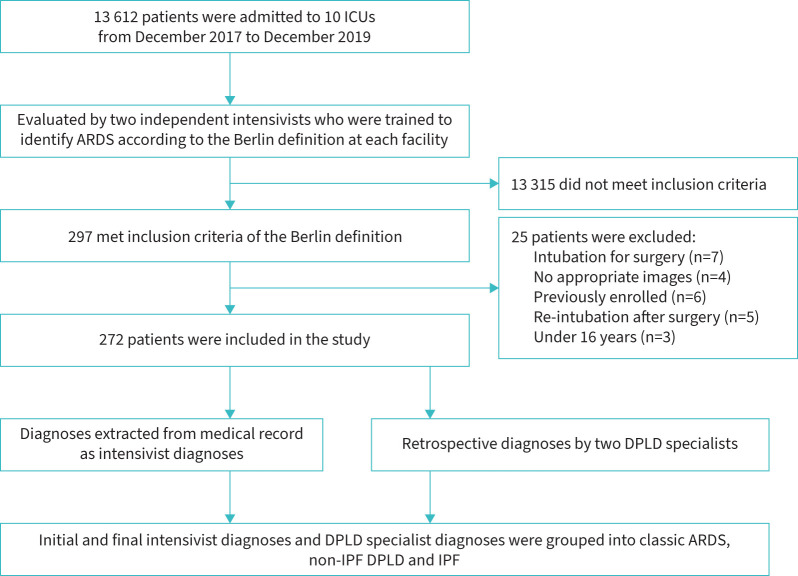
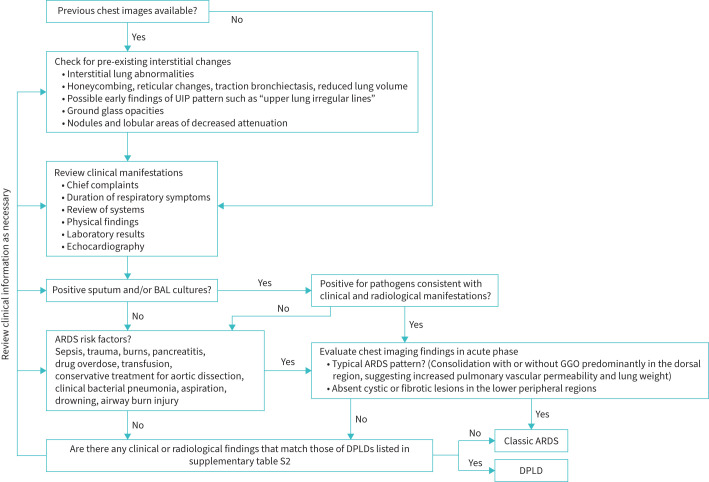
Methods: This Japan-based multicentre retrospective cohort study included patients on mechanical ventilation who met the Berlin definition. For all participants, diagnosis was made by pulmonology specialists in DPLD and thoracic radiology (blinded to clinical diagnoses) by reviewing an extensive database designed for DPLD diagnosis across 10 participating hospitals.
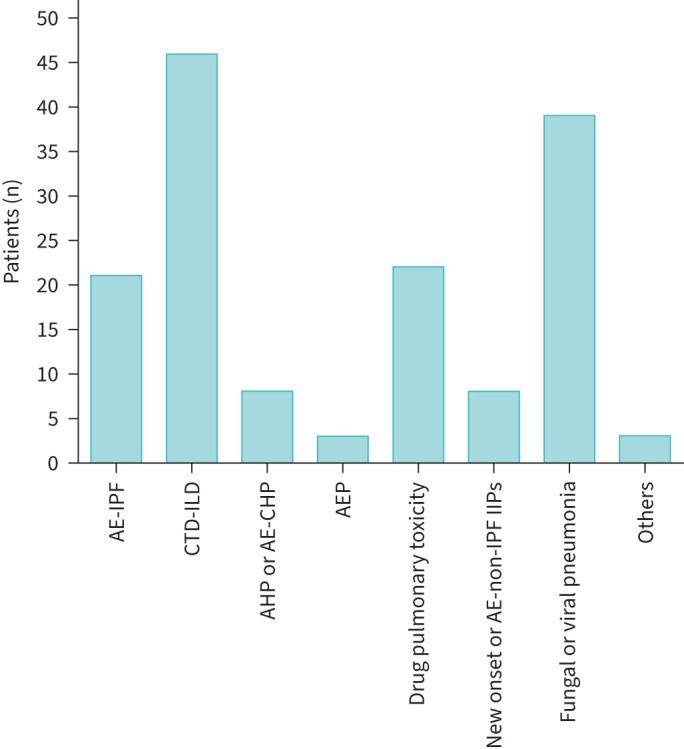
Results: Of 13 612 patients admitted to the intensive care unit during the study period, 272 met the Berlin definition of ARDS and were included for analysis. All underwent at least one chest computed tomography scan; none underwent lung biopsy. Briefly, 182 were designated classic ARDS (67%), 69 non-IPF (idiopathic pulmonary fibrosis) DPLDs (25%) and 21 IPF (8%) by DPLD specialists. Of the 90 patients diagnosed with DPLD (IPF or non-IPF) by specialists, 35% were diagnosed with classic ARDS by intensivists at the end of the clinical course. Diagnostic classifications of classic ARDS and IPF by DPLD specialists were associated with time-to-death (adjusted hazard ratio (HR) 1.58 (95% CI 1.03-2.45), p=0.038, and adjusted HR 1.73 (95% CI 1.01-2.97), p=0.045, respectively) and in-hospital mortality (adjusted HR 1.54 (95% CI 1.06-2.23), p=0.022 for classic ARDS) versus non-IPF DPLDs; intensivist diagnostic classifications were not.
Conclusion: Approximately one-third of patients within the Berlin definition were retrospectively diagnosed with new-onset or acutely exacerbated DPLD by specialists.
期刊介绍:
ERJ Open Research is a fully open access original research journal, published online by the European Respiratory Society. The journal aims to publish high-quality work in all fields of respiratory science and medicine, covering basic science, clinical translational science and clinical medicine. The journal was created to help fulfil the ERS objective to disseminate scientific and educational material to its members and to the medical community, but also to provide researchers with an affordable open access specialty journal in which to publish their work.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


