{"title":"Graves病合并IID型假性醛固酮减少症1例报告。","authors":"Junlan Yao, Xiangji Li, Wei Lu","doi":"10.21037/tp-2025-500","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Graves' disease and pseudohypoaldosteronism type IID (PHA IID) are rare pediatric endocrine diseases with different etiologies and pathological features. Graves' disease is caused by autoimmune thyroid stimulation, while PHA IID is an inherited renal tubular disorder characterized by hyperkalemia and hypertension due to mutations in the <i>KLHL3</i> gene. A rare pediatric case of concurrent Graves' disease and PHA IID with a <i>KLHL3</i> gene mutation is reported. The clinical manifestations, diagnostic process, and treatment plans for the two conditions are discussed to provide a reference for the management of similar cases.</p><p><strong>Case description: </strong>On the initial hospitalization, the patient presented with sudden onset of altered consciousness, tachycardia, and electrolyte disturbances, including hyperkalemia and metabolic acidosis. Following thyroid function tests and thyroid ultrasonography, a diagnosis of Graves' disease was made. Antithyroid treatment with methimazole and propranolol was administered, leading to an improvement in the blood gas and biochemical parameters. Although thyroid function was controlled, the patient's hyperkalemia, hyperchloremia, metabolic acidosis, and hypertension remained refractory to treatment. Further genetic testing revealed a <i>KLHL3</i> gene mutation, confirming the diagnosis of PHA IID. After treatment with hydrochlorothiazide (10 mg), the patient's electrolyte imbalances and blood pressure normalized.</p><p><strong>Conclusions: </strong>The simultaneous occurrence of Graves' disease and PHA IID is rare in children. Clinicians should be alert to the possibility of such comorbidities in clinical practice. For patients with persistent hyperkalemia, particularly those with concomitant metabolic acidosis and hyperchloremia, early genetic testing can enhance diagnostic efficiency and optimize treatment strategies.</p>","PeriodicalId":23294,"journal":{"name":"Translational pediatrics","volume":"14 8","pages":"2066-2074"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433029/pdf/","citationCount":"0","resultStr":"{\"title\":\"A case report of Graves' disease combined with pseudohypoaldosteronism type IID in a child.\",\"authors\":\"Junlan Yao, Xiangji Li, Wei Lu\",\"doi\":\"10.21037/tp-2025-500\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Graves' disease and pseudohypoaldosteronism type IID (PHA IID) are rare pediatric endocrine diseases with different etiologies and pathological features. Graves' disease is caused by autoimmune thyroid stimulation, while PHA IID is an inherited renal tubular disorder characterized by hyperkalemia and hypertension due to mutations in the <i>KLHL3</i> gene. A rare pediatric case of concurrent Graves' disease and PHA IID with a <i>KLHL3</i> gene mutation is reported. The clinical manifestations, diagnostic process, and treatment plans for the two conditions are discussed to provide a reference for the management of similar cases.</p><p><strong>Case description: </strong>On the initial hospitalization, the patient presented with sudden onset of altered consciousness, tachycardia, and electrolyte disturbances, including hyperkalemia and metabolic acidosis. Following thyroid function tests and thyroid ultrasonography, a diagnosis of Graves' disease was made. Antithyroid treatment with methimazole and propranolol was administered, leading to an improvement in the blood gas and biochemical parameters. Although thyroid function was controlled, the patient's hyperkalemia, hyperchloremia, metabolic acidosis, and hypertension remained refractory to treatment. Further genetic testing revealed a <i>KLHL3</i> gene mutation, confirming the diagnosis of PHA IID. After treatment with hydrochlorothiazide (10 mg), the patient's electrolyte imbalances and blood pressure normalized.</p><p><strong>Conclusions: </strong>The simultaneous occurrence of Graves' disease and PHA IID is rare in children. Clinicians should be alert to the possibility of such comorbidities in clinical practice. For patients with persistent hyperkalemia, particularly those with concomitant metabolic acidosis and hyperchloremia, early genetic testing can enhance diagnostic efficiency and optimize treatment strategies.</p>\",\"PeriodicalId\":23294,\"journal\":{\"name\":\"Translational pediatrics\",\"volume\":\"14 8\",\"pages\":\"2066-2074\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433029/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational pediatrics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/tp-2025-500\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tp-2025-500","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
A case report of Graves' disease combined with pseudohypoaldosteronism type IID in a child.
Background: Graves' disease and pseudohypoaldosteronism type IID (PHA IID) are rare pediatric endocrine diseases with different etiologies and pathological features. Graves' disease is caused by autoimmune thyroid stimulation, while PHA IID is an inherited renal tubular disorder characterized by hyperkalemia and hypertension due to mutations in the KLHL3 gene. A rare pediatric case of concurrent Graves' disease and PHA IID with a KLHL3 gene mutation is reported. The clinical manifestations, diagnostic process, and treatment plans for the two conditions are discussed to provide a reference for the management of similar cases.
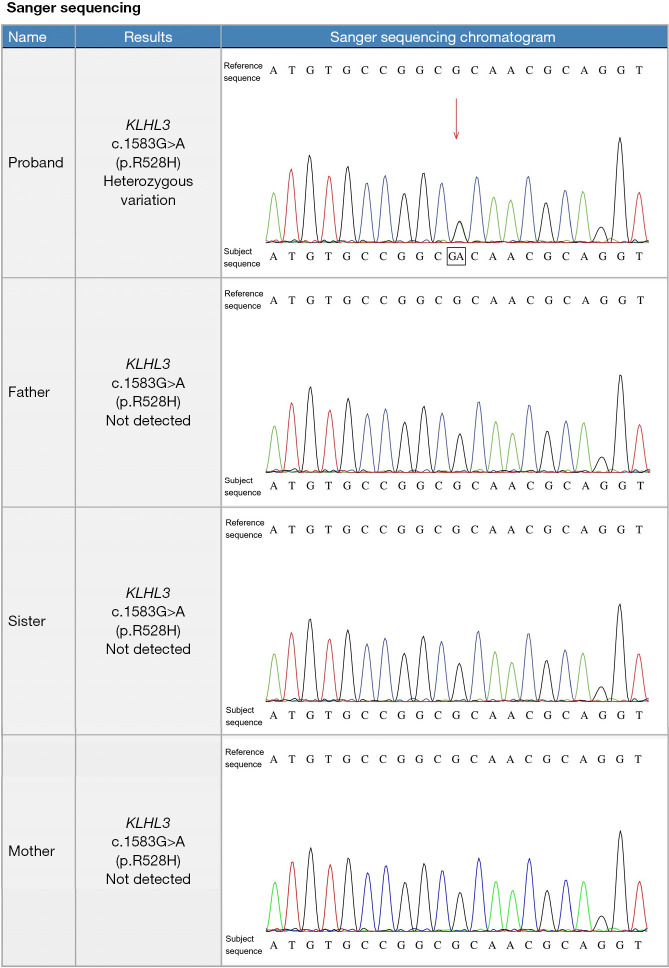
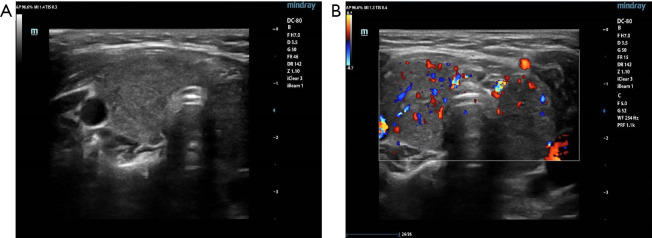
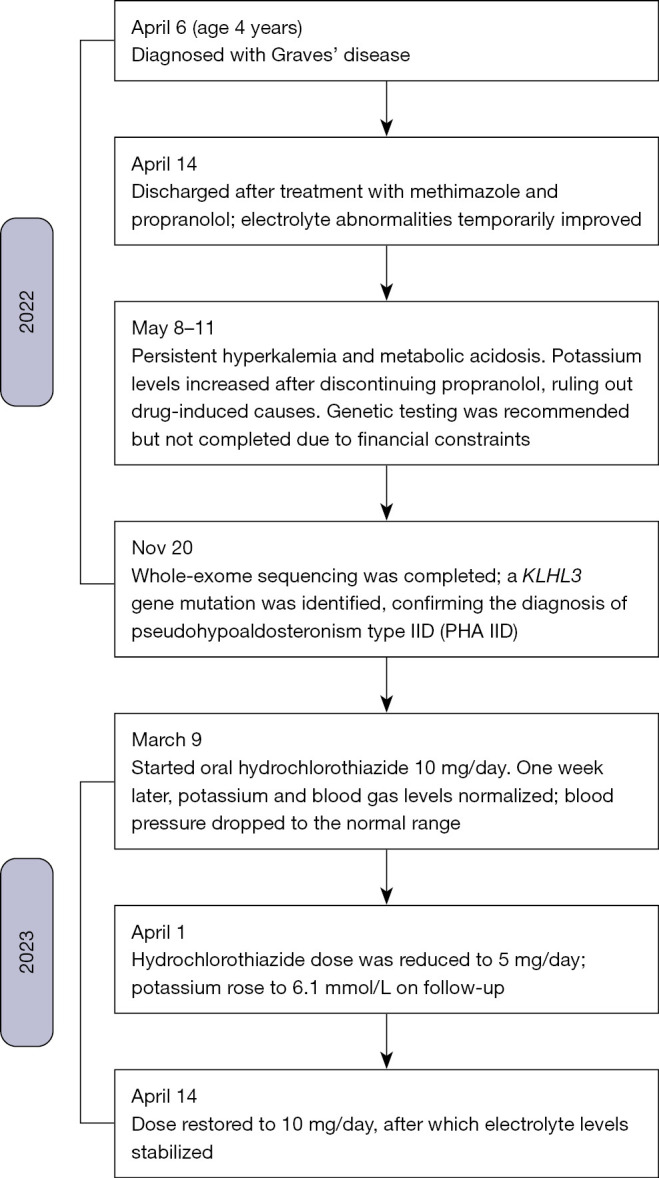
Case description: On the initial hospitalization, the patient presented with sudden onset of altered consciousness, tachycardia, and electrolyte disturbances, including hyperkalemia and metabolic acidosis. Following thyroid function tests and thyroid ultrasonography, a diagnosis of Graves' disease was made. Antithyroid treatment with methimazole and propranolol was administered, leading to an improvement in the blood gas and biochemical parameters. Although thyroid function was controlled, the patient's hyperkalemia, hyperchloremia, metabolic acidosis, and hypertension remained refractory to treatment. Further genetic testing revealed a KLHL3 gene mutation, confirming the diagnosis of PHA IID. After treatment with hydrochlorothiazide (10 mg), the patient's electrolyte imbalances and blood pressure normalized.
Conclusions: The simultaneous occurrence of Graves' disease and PHA IID is rare in children. Clinicians should be alert to the possibility of such comorbidities in clinical practice. For patients with persistent hyperkalemia, particularly those with concomitant metabolic acidosis and hyperchloremia, early genetic testing can enhance diagnostic efficiency and optimize treatment strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


