Jaejung Ryu, Bum-Sik Lee, Jong-Min Kim, Ju-Ho Song, Ho Yeon Kim
{"title":"内侧骨关节炎膝关节截骨术后关节线过度倾斜的影像学危险因素:一种基于表型的方法。","authors":"Jaejung Ryu, Bum-Sik Lee, Jong-Min Kim, Ju-Ho Song, Ho Yeon Kim","doi":"10.1177/23259671251351335","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients undergoing high tibial osteotomy (HTO), an excessive increase in joint line obliquity (JLO) after surgery leads to poor clinical outcomes. Phenotype analysis is a simple and intuitive method to classify knee alignment, including JLO. However, there are no studies investigating phenotype changes before and after surgery in patients undergoing realignment osteotomy.</p><p><strong>Purpose: </strong>To investigate (1) the preoperative and postoperative phenotype distribution in patients undergoing primary realignment osteotomy for medial compartmental osteoarthritis and (2) the incidence and radiographic risk factors for excessive postoperative JLO.</p><p><strong>Study design: </strong>Cross-sectional study; Level of evidence, 3.</p><p><strong>Methods: </strong>A total of 348 knees (320 patients) undergoing primary realignment osteotomy for medial compartmental osteoarthritis with a varus deformity from January 2010 to July 2021 were included. Preoperatively and at 1 year postoperatively, we evaluated coronal-plane alignment on standing scanograms, classifying them into 9 phenotypes based on the modified Coronal Plane Alignment of the Knee classification. We identified changes in the preoperative and postoperative phenotype distribution through scatterplots and analyzed differences in excessive postoperative JLO (arithmetic JLO [aJLO] >4°) based on the preoperative phenotype. Receiver operating characteristic analysis identified preoperative radiographic parameters and their cut-off values as risk factors for excessive postoperative JLO after HTO.</p><p><strong>Results: </strong>The most common preoperative phenotype was type I (varus and apex distal; n = 149 [42.8%]), and the most common postoperative phenotype was type VI (valgus and apex neutral; n = 187 [53.7%]). The incidence of excessive postoperative JLO was significantly higher in preoperative type IV (varus and apex neutral; 14.5%) than in type I (0.7%), type II (neutral and apex distal; 0.0%), and type V (neutral and apex neutral; 10.4%). In receiver operating characteristic analysis for excessive postoperative JLO, the preoperative mechanical lateral distal femoral angle (mLDFA) and aJLO showed a high area under the curve of 0.916 and 0.914, respectively, with cut-off values of 90.2° and -1.5°, respectively. In the preoperative mLDFA ≥90.2° group, the incidence of excessive postoperative JLO was significantly higher than in the preoperative mLDFA <90.2° group (19.8% vs 0.4%, respectively; <i>P</i> < .001). In the preoperative aJLO ≥-1.5° group, the incidence of excessive postoperative JLO was significantly higher than in the preoperative aJLO <-1.5° group (35.1% vs 1.4%, respectively; <i>P</i> < .001).</p><p><strong>Conclusion: </strong>Preoperative type IV (varus and apex neutral) had a higher risk of excessive postoperative JLO. Specifically, when the preoperative mLDFA was ≥90.2° or the preoperative aJLO was ≥-1.5°, there was an increased risk of excessive postoperative JLO after isolated HTO.</p>","PeriodicalId":19646,"journal":{"name":"Orthopaedic Journal of Sports Medicine","volume":"13 9","pages":"23259671251351335"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432296/pdf/","citationCount":"0","resultStr":"{\"title\":\"Radiographic Risk Factors for Excessive Joint Line Obliquity After Knee Osteotomy for Medial Osteoarthritis: A Phenotype-Based Approach.\",\"authors\":\"Jaejung Ryu, Bum-Sik Lee, Jong-Min Kim, Ju-Ho Song, Ho Yeon Kim\",\"doi\":\"10.1177/23259671251351335\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In patients undergoing high tibial osteotomy (HTO), an excessive increase in joint line obliquity (JLO) after surgery leads to poor clinical outcomes. Phenotype analysis is a simple and intuitive method to classify knee alignment, including JLO. However, there are no studies investigating phenotype changes before and after surgery in patients undergoing realignment osteotomy.</p><p><strong>Purpose: </strong>To investigate (1) the preoperative and postoperative phenotype distribution in patients undergoing primary realignment osteotomy for medial compartmental osteoarthritis and (2) the incidence and radiographic risk factors for excessive postoperative JLO.</p><p><strong>Study design: </strong>Cross-sectional study; Level of evidence, 3.</p><p><strong>Methods: </strong>A total of 348 knees (320 patients) undergoing primary realignment osteotomy for medial compartmental osteoarthritis with a varus deformity from January 2010 to July 2021 were included. Preoperatively and at 1 year postoperatively, we evaluated coronal-plane alignment on standing scanograms, classifying them into 9 phenotypes based on the modified Coronal Plane Alignment of the Knee classification. We identified changes in the preoperative and postoperative phenotype distribution through scatterplots and analyzed differences in excessive postoperative JLO (arithmetic JLO [aJLO] >4°) based on the preoperative phenotype. Receiver operating characteristic analysis identified preoperative radiographic parameters and their cut-off values as risk factors for excessive postoperative JLO after HTO.</p><p><strong>Results: </strong>The most common preoperative phenotype was type I (varus and apex distal; n = 149 [42.8%]), and the most common postoperative phenotype was type VI (valgus and apex neutral; n = 187 [53.7%]). The incidence of excessive postoperative JLO was significantly higher in preoperative type IV (varus and apex neutral; 14.5%) than in type I (0.7%), type II (neutral and apex distal; 0.0%), and type V (neutral and apex neutral; 10.4%). In receiver operating characteristic analysis for excessive postoperative JLO, the preoperative mechanical lateral distal femoral angle (mLDFA) and aJLO showed a high area under the curve of 0.916 and 0.914, respectively, with cut-off values of 90.2° and -1.5°, respectively. In the preoperative mLDFA ≥90.2° group, the incidence of excessive postoperative JLO was significantly higher than in the preoperative mLDFA <90.2° group (19.8% vs 0.4%, respectively; <i>P</i> < .001). In the preoperative aJLO ≥-1.5° group, the incidence of excessive postoperative JLO was significantly higher than in the preoperative aJLO <-1.5° group (35.1% vs 1.4%, respectively; <i>P</i> < .001).</p><p><strong>Conclusion: </strong>Preoperative type IV (varus and apex neutral) had a higher risk of excessive postoperative JLO. Specifically, when the preoperative mLDFA was ≥90.2° or the preoperative aJLO was ≥-1.5°, there was an increased risk of excessive postoperative JLO after isolated HTO.</p>\",\"PeriodicalId\":19646,\"journal\":{\"name\":\"Orthopaedic Journal of Sports Medicine\",\"volume\":\"13 9\",\"pages\":\"23259671251351335\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-09-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432296/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Orthopaedic Journal of Sports Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/23259671251351335\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Orthopaedic Journal of Sports Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/23259671251351335","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Radiographic Risk Factors for Excessive Joint Line Obliquity After Knee Osteotomy for Medial Osteoarthritis: A Phenotype-Based Approach.
Background: In patients undergoing high tibial osteotomy (HTO), an excessive increase in joint line obliquity (JLO) after surgery leads to poor clinical outcomes. Phenotype analysis is a simple and intuitive method to classify knee alignment, including JLO. However, there are no studies investigating phenotype changes before and after surgery in patients undergoing realignment osteotomy.
Purpose: To investigate (1) the preoperative and postoperative phenotype distribution in patients undergoing primary realignment osteotomy for medial compartmental osteoarthritis and (2) the incidence and radiographic risk factors for excessive postoperative JLO.
Study design: Cross-sectional study; Level of evidence, 3.
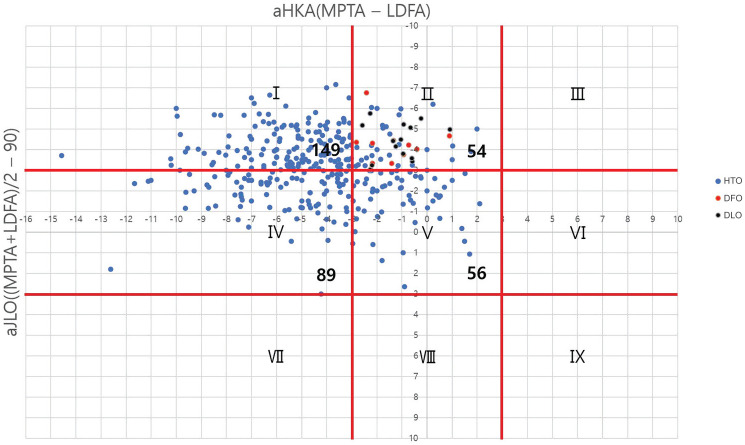
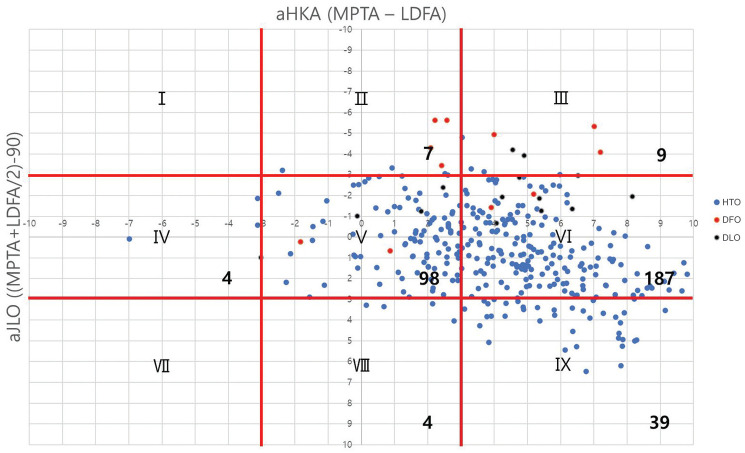
Methods: A total of 348 knees (320 patients) undergoing primary realignment osteotomy for medial compartmental osteoarthritis with a varus deformity from January 2010 to July 2021 were included. Preoperatively and at 1 year postoperatively, we evaluated coronal-plane alignment on standing scanograms, classifying them into 9 phenotypes based on the modified Coronal Plane Alignment of the Knee classification. We identified changes in the preoperative and postoperative phenotype distribution through scatterplots and analyzed differences in excessive postoperative JLO (arithmetic JLO [aJLO] >4°) based on the preoperative phenotype. Receiver operating characteristic analysis identified preoperative radiographic parameters and their cut-off values as risk factors for excessive postoperative JLO after HTO.
Results: The most common preoperative phenotype was type I (varus and apex distal; n = 149 [42.8%]), and the most common postoperative phenotype was type VI (valgus and apex neutral; n = 187 [53.7%]). The incidence of excessive postoperative JLO was significantly higher in preoperative type IV (varus and apex neutral; 14.5%) than in type I (0.7%), type II (neutral and apex distal; 0.0%), and type V (neutral and apex neutral; 10.4%). In receiver operating characteristic analysis for excessive postoperative JLO, the preoperative mechanical lateral distal femoral angle (mLDFA) and aJLO showed a high area under the curve of 0.916 and 0.914, respectively, with cut-off values of 90.2° and -1.5°, respectively. In the preoperative mLDFA ≥90.2° group, the incidence of excessive postoperative JLO was significantly higher than in the preoperative mLDFA <90.2° group (19.8% vs 0.4%, respectively; P < .001). In the preoperative aJLO ≥-1.5° group, the incidence of excessive postoperative JLO was significantly higher than in the preoperative aJLO <-1.5° group (35.1% vs 1.4%, respectively; P < .001).
Conclusion: Preoperative type IV (varus and apex neutral) had a higher risk of excessive postoperative JLO. Specifically, when the preoperative mLDFA was ≥90.2° or the preoperative aJLO was ≥-1.5°, there was an increased risk of excessive postoperative JLO after isolated HTO.
期刊介绍:
The Orthopaedic Journal of Sports Medicine (OJSM), developed by the American Orthopaedic Society for Sports Medicine (AOSSM), is a global, peer-reviewed, open access journal that combines the interests of researchers and clinical practitioners across orthopaedic sports medicine, arthroscopy, and knee arthroplasty.
Topics include original research in the areas of:
-Orthopaedic Sports Medicine, including surgical and nonsurgical treatment of orthopaedic sports injuries
-Arthroscopic Surgery (Shoulder/Elbow/Wrist/Hip/Knee/Ankle/Foot)
-Relevant translational research
-Sports traumatology/epidemiology
-Knee and shoulder arthroplasty
The OJSM also publishes relevant systematic reviews and meta-analyses.
This journal is a member of the Committee on Publication Ethics (COPE).


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


