Stefanie Meiler, Daniel Schmalenberger, Maximilian Malfertheiner, Iris Dvorak, Quirin Strotzer, Christian Stroszczynski, Okka Wilkea Hamer
{"title":"胸部计算机断层扫描结果不影响肺病学家对肺部长冠状病毒病的诊断和治疗的决定:一项单中心回顾性研究","authors":"Stefanie Meiler, Daniel Schmalenberger, Maximilian Malfertheiner, Iris Dvorak, Quirin Strotzer, Christian Stroszczynski, Okka Wilkea Hamer","doi":"10.21037/jtd-2025-433","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pulmonary symptoms are common in long coronavirus disease (COVID), yet the diagnostic value of chest computed tomography (CT) in these patients remains unclear, particularly when physical examination and pulmonary function tests are normal. This study investigates whether chest CT influences the decision of pneumologists regarding the measures taken for diagnostic work-up, the final diagnosis, the confidence in the diagnosis, and the downstream management of patients suspected to suffer from pulmonary long COVID.</p><p><strong>Methods: </strong>All patients presented in a dedicated long COVID outpatient clinic of a secondary care hospital that specializes in lung diseases between April 2020 and August 2021. Inclusion criteria were age ≥18 years, suspicion for long COVID syndrome of pulmonary origin according to the National Institute for Health and Care Excellence (NICE) criteria and availability of a chest CT acquired during work-up. Three pneumologists evaluated the patient's records in two rounds (round 1 without and round 2 with knowledge of CT results). Identical parameters were queried in the two runs: diagnosis of pulmonary long COVID, confidence of the diagnosis on a scale from 0 to 3, need for: bronchoalveolar lavage (BAL), transbronchial biopsy (TBB), cryobiopsy, video-assisted thoracoscopy (VATS), ergospirometry, ventilation/perfusion scintigraphy, follow-up appointment, rehabilitation.</p><p><strong>Results: </strong>Forty-one patients were included (24 male; age 21 to 72 years, mean 55 years). In the first and second round diagnosis of pulmonary long COVID was made in an average of 10 (24%) and 11 (27%) patients (P=0.69). Confidence of diagnosis was 1.9 and 2.6 (P<0.001). No statistical difference was found regarding the frequency of diagnostic measures and downstream management.</p><p><strong>Conclusions: </strong>Chest CT did not influence the diagnostic decision of pneumologists for patients suspected to suffer from pulmonary long COVID. However, the confidence in the diagnosis was improved by chest CT. Still, based on our results chest CT does not routinely have to be included in the work-up of long COVID, when pulmonary function tests and auscultation are normal.</p>","PeriodicalId":17542,"journal":{"name":"Journal of thoracic disease","volume":"17 8","pages":"5654-5662"},"PeriodicalIF":1.9000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433019/pdf/","citationCount":"0","resultStr":"{\"title\":\"Chest computed tomography findings do not influence the decision of pneumologists regarding the diagnosis and management of pulmonary long coronavirus disease: a single center retrospective study.\",\"authors\":\"Stefanie Meiler, Daniel Schmalenberger, Maximilian Malfertheiner, Iris Dvorak, Quirin Strotzer, Christian Stroszczynski, Okka Wilkea Hamer\",\"doi\":\"10.21037/jtd-2025-433\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pulmonary symptoms are common in long coronavirus disease (COVID), yet the diagnostic value of chest computed tomography (CT) in these patients remains unclear, particularly when physical examination and pulmonary function tests are normal. This study investigates whether chest CT influences the decision of pneumologists regarding the measures taken for diagnostic work-up, the final diagnosis, the confidence in the diagnosis, and the downstream management of patients suspected to suffer from pulmonary long COVID.</p><p><strong>Methods: </strong>All patients presented in a dedicated long COVID outpatient clinic of a secondary care hospital that specializes in lung diseases between April 2020 and August 2021. Inclusion criteria were age ≥18 years, suspicion for long COVID syndrome of pulmonary origin according to the National Institute for Health and Care Excellence (NICE) criteria and availability of a chest CT acquired during work-up. Three pneumologists evaluated the patient's records in two rounds (round 1 without and round 2 with knowledge of CT results). Identical parameters were queried in the two runs: diagnosis of pulmonary long COVID, confidence of the diagnosis on a scale from 0 to 3, need for: bronchoalveolar lavage (BAL), transbronchial biopsy (TBB), cryobiopsy, video-assisted thoracoscopy (VATS), ergospirometry, ventilation/perfusion scintigraphy, follow-up appointment, rehabilitation.</p><p><strong>Results: </strong>Forty-one patients were included (24 male; age 21 to 72 years, mean 55 years). In the first and second round diagnosis of pulmonary long COVID was made in an average of 10 (24%) and 11 (27%) patients (P=0.69). Confidence of diagnosis was 1.9 and 2.6 (P<0.001). No statistical difference was found regarding the frequency of diagnostic measures and downstream management.</p><p><strong>Conclusions: </strong>Chest CT did not influence the diagnostic decision of pneumologists for patients suspected to suffer from pulmonary long COVID. However, the confidence in the diagnosis was improved by chest CT. Still, based on our results chest CT does not routinely have to be included in the work-up of long COVID, when pulmonary function tests and auscultation are normal.</p>\",\"PeriodicalId\":17542,\"journal\":{\"name\":\"Journal of thoracic disease\",\"volume\":\"17 8\",\"pages\":\"5654-5662\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433019/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of thoracic disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/jtd-2025-433\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of thoracic disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/jtd-2025-433","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Chest computed tomography findings do not influence the decision of pneumologists regarding the diagnosis and management of pulmonary long coronavirus disease: a single center retrospective study.
Background: Pulmonary symptoms are common in long coronavirus disease (COVID), yet the diagnostic value of chest computed tomography (CT) in these patients remains unclear, particularly when physical examination and pulmonary function tests are normal. This study investigates whether chest CT influences the decision of pneumologists regarding the measures taken for diagnostic work-up, the final diagnosis, the confidence in the diagnosis, and the downstream management of patients suspected to suffer from pulmonary long COVID.
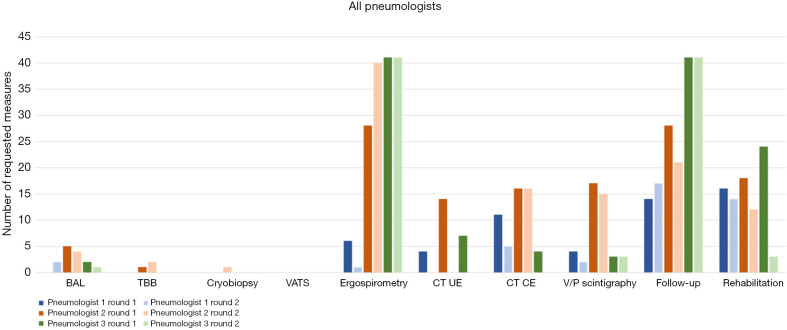
Methods: All patients presented in a dedicated long COVID outpatient clinic of a secondary care hospital that specializes in lung diseases between April 2020 and August 2021. Inclusion criteria were age ≥18 years, suspicion for long COVID syndrome of pulmonary origin according to the National Institute for Health and Care Excellence (NICE) criteria and availability of a chest CT acquired during work-up. Three pneumologists evaluated the patient's records in two rounds (round 1 without and round 2 with knowledge of CT results). Identical parameters were queried in the two runs: diagnosis of pulmonary long COVID, confidence of the diagnosis on a scale from 0 to 3, need for: bronchoalveolar lavage (BAL), transbronchial biopsy (TBB), cryobiopsy, video-assisted thoracoscopy (VATS), ergospirometry, ventilation/perfusion scintigraphy, follow-up appointment, rehabilitation.
Results: Forty-one patients were included (24 male; age 21 to 72 years, mean 55 years). In the first and second round diagnosis of pulmonary long COVID was made in an average of 10 (24%) and 11 (27%) patients (P=0.69). Confidence of diagnosis was 1.9 and 2.6 (P<0.001). No statistical difference was found regarding the frequency of diagnostic measures and downstream management.
Conclusions: Chest CT did not influence the diagnostic decision of pneumologists for patients suspected to suffer from pulmonary long COVID. However, the confidence in the diagnosis was improved by chest CT. Still, based on our results chest CT does not routinely have to be included in the work-up of long COVID, when pulmonary function tests and auscultation are normal.
期刊介绍:
The Journal of Thoracic Disease (JTD, J Thorac Dis, pISSN: 2072-1439; eISSN: 2077-6624) was founded in Dec 2009, and indexed in PubMed in Dec 2011 and Science Citation Index SCI in Feb 2013. It is published quarterly (Dec 2009- Dec 2011), bimonthly (Jan 2012 - Dec 2013), monthly (Jan. 2014-) and openly distributed worldwide. JTD received its impact factor of 2.365 for the year 2016. JTD publishes manuscripts that describe new findings and provide current, practical information on the diagnosis and treatment of conditions related to thoracic disease. All the submission and reviewing are conducted electronically so that rapid review is assured.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


