{"title":"早期低her -2乳腺癌新辅助化疗疗效的影响因素及病理完全缓解的预测模型","authors":"Shuai Duan, Dilimulati Aisimutula, Yiyang Wang, Binjie Zheng, Chenming Guo","doi":"10.21037/gs-2025-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>At present, human epidermal growth factor receptor 2 (HER-2)-low and HER-2-zero breast cancer (BC) are still classified into a single category, which simplifies targeting in the selection of neoadjuvant chemotherapy (NAC) regimens. Moreover, no studies have reported the factors influencing pathological complete response (pCR) after NAC for HER-2-low early-stage breast cancer (eBC) and constructed predictive models. This study aimed to clarify the tumor heterogeneity of these two types of eBC to provide a research basis for subsequent clinical classification and diagnosis. Moreover, a prediction model was constructed to provide a basis for the selection of the initial treatment plan for HER-2-low eBC.</p><p><strong>Methods: </strong>This study retrospectively included 212 patients with HER-2-low and HER-2-zero eBC treated with NAC and surgery from April 2013 to March 2024. The differences in the effects of NAC were compared at the imaging and pathological levels via Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and the Miller-Payne assessment criteria, and the clinical and core needle biopsy histopathological (CNB) features were analyzed to clarify the influencing factors. Moreover, the clinical and pathological factors influencing pCR after NAC for HER-2-low eBC were analyzed via univariate analysis and multifactorial binary logistic regression. A nomogram prediction model was constructed based on the independent influencing factors, diagnostic calibration curves were used for the goodness-of-fit test, and the performance of the prediction model was evaluated via receiver operating characteristic (ROC) curve analysis.</p><p><strong>Results: </strong>HER-2-low eBC was associated with worse responsiveness to NAC at both the imaging and pathologic levels (P<0.05) and were significantly associated with estrogen receptor (ER)-positive status (P=0.03), progesterone receptor (PR)-positive status (P=0.04), and a low expression of Ki-67 (P=0.045). Univariate analysis indicated that a maximum tumor diameter >3 cm (P=0.04), positive axillary lymph nodes through puncture (P=0.001), fewer chemotherapeutic cycles (P=0.002), pathological grading I or II through puncture (P=0.04), ER-positive status (P=0.001), PR-positive status (P<0.001), low expression of Ki-67 (P=0.04), androgen receptor (AR)-positive status (P<0.001), and tumor invasion (P=0.002) were all unfavorable factors influencing pCR after NAC of HER-2-low eBC. Multifactorial analysis found that a maximum tumor diameter >3 cm [odds ratio (OR): 0.088; 95% confidence interval (CI): 0.015-0.529; P=0.008], positive axillary lymph nodes through puncture (OR: 18.677; 95% CI: 3.028-115.201; P=0.002), and fewer chemotherapeutic cycles (OR: 0.337; 95% CI: 0.148-0.764; P=0.009) were independent unfavorable factors. The area under the ROC of the nomogram prediction model for pCR after NAC for HER-2-low eBC was 0.861 (95% CI: 0.785-0.936), with a sensitivity of 80.0% and a specificity of 77.1%.</p><p><strong>Conclusions: </strong>HER-2-low and HER-2-zero eBC respond differently to NAC and may need to be categorized in the future. Whether pCR can be achieved after NAC for HER-2-low eBC is influenced by multiple factors, and the nomogram prediction model has certain clinical prediction value.</p>","PeriodicalId":12760,"journal":{"name":"Gland surgery","volume":"14 8","pages":"1418-1432"},"PeriodicalIF":1.6000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432962/pdf/","citationCount":"0","resultStr":"{\"title\":\"Factors influencing the efficacy of neoadjuvant chemotherapy for HER-2-low early-stage breast cancer and a predictive model for pathological complete response.\",\"authors\":\"Shuai Duan, Dilimulati Aisimutula, Yiyang Wang, Binjie Zheng, Chenming Guo\",\"doi\":\"10.21037/gs-2025-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>At present, human epidermal growth factor receptor 2 (HER-2)-low and HER-2-zero breast cancer (BC) are still classified into a single category, which simplifies targeting in the selection of neoadjuvant chemotherapy (NAC) regimens. Moreover, no studies have reported the factors influencing pathological complete response (pCR) after NAC for HER-2-low early-stage breast cancer (eBC) and constructed predictive models. This study aimed to clarify the tumor heterogeneity of these two types of eBC to provide a research basis for subsequent clinical classification and diagnosis. Moreover, a prediction model was constructed to provide a basis for the selection of the initial treatment plan for HER-2-low eBC.</p><p><strong>Methods: </strong>This study retrospectively included 212 patients with HER-2-low and HER-2-zero eBC treated with NAC and surgery from April 2013 to March 2024. The differences in the effects of NAC were compared at the imaging and pathological levels via Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and the Miller-Payne assessment criteria, and the clinical and core needle biopsy histopathological (CNB) features were analyzed to clarify the influencing factors. Moreover, the clinical and pathological factors influencing pCR after NAC for HER-2-low eBC were analyzed via univariate analysis and multifactorial binary logistic regression. A nomogram prediction model was constructed based on the independent influencing factors, diagnostic calibration curves were used for the goodness-of-fit test, and the performance of the prediction model was evaluated via receiver operating characteristic (ROC) curve analysis.</p><p><strong>Results: </strong>HER-2-low eBC was associated with worse responsiveness to NAC at both the imaging and pathologic levels (P<0.05) and were significantly associated with estrogen receptor (ER)-positive status (P=0.03), progesterone receptor (PR)-positive status (P=0.04), and a low expression of Ki-67 (P=0.045). Univariate analysis indicated that a maximum tumor diameter >3 cm (P=0.04), positive axillary lymph nodes through puncture (P=0.001), fewer chemotherapeutic cycles (P=0.002), pathological grading I or II through puncture (P=0.04), ER-positive status (P=0.001), PR-positive status (P<0.001), low expression of Ki-67 (P=0.04), androgen receptor (AR)-positive status (P<0.001), and tumor invasion (P=0.002) were all unfavorable factors influencing pCR after NAC of HER-2-low eBC. Multifactorial analysis found that a maximum tumor diameter >3 cm [odds ratio (OR): 0.088; 95% confidence interval (CI): 0.015-0.529; P=0.008], positive axillary lymph nodes through puncture (OR: 18.677; 95% CI: 3.028-115.201; P=0.002), and fewer chemotherapeutic cycles (OR: 0.337; 95% CI: 0.148-0.764; P=0.009) were independent unfavorable factors. The area under the ROC of the nomogram prediction model for pCR after NAC for HER-2-low eBC was 0.861 (95% CI: 0.785-0.936), with a sensitivity of 80.0% and a specificity of 77.1%.</p><p><strong>Conclusions: </strong>HER-2-low and HER-2-zero eBC respond differently to NAC and may need to be categorized in the future. Whether pCR can be achieved after NAC for HER-2-low eBC is influenced by multiple factors, and the nomogram prediction model has certain clinical prediction value.</p>\",\"PeriodicalId\":12760,\"journal\":{\"name\":\"Gland surgery\",\"volume\":\"14 8\",\"pages\":\"1418-1432\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432962/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gland surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/gs-2025-7\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gland surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/gs-2025-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Factors influencing the efficacy of neoadjuvant chemotherapy for HER-2-low early-stage breast cancer and a predictive model for pathological complete response.
Background: At present, human epidermal growth factor receptor 2 (HER-2)-low and HER-2-zero breast cancer (BC) are still classified into a single category, which simplifies targeting in the selection of neoadjuvant chemotherapy (NAC) regimens. Moreover, no studies have reported the factors influencing pathological complete response (pCR) after NAC for HER-2-low early-stage breast cancer (eBC) and constructed predictive models. This study aimed to clarify the tumor heterogeneity of these two types of eBC to provide a research basis for subsequent clinical classification and diagnosis. Moreover, a prediction model was constructed to provide a basis for the selection of the initial treatment plan for HER-2-low eBC.
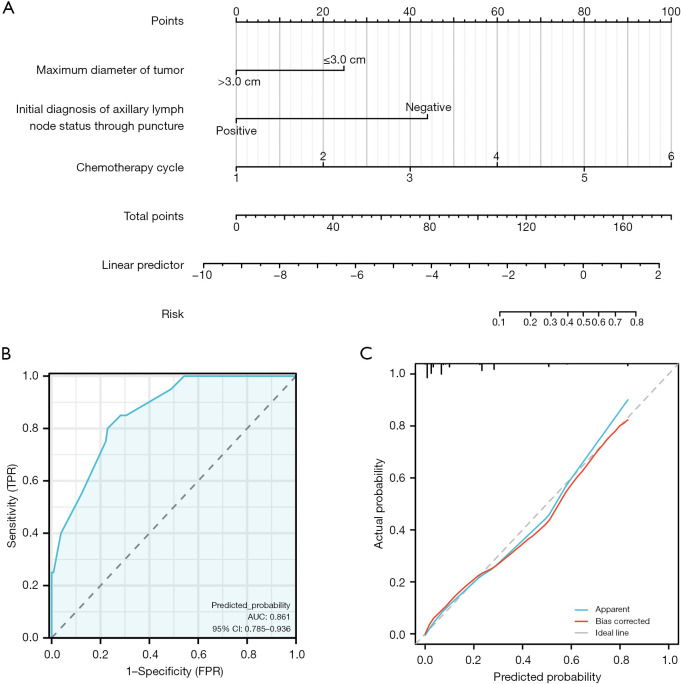
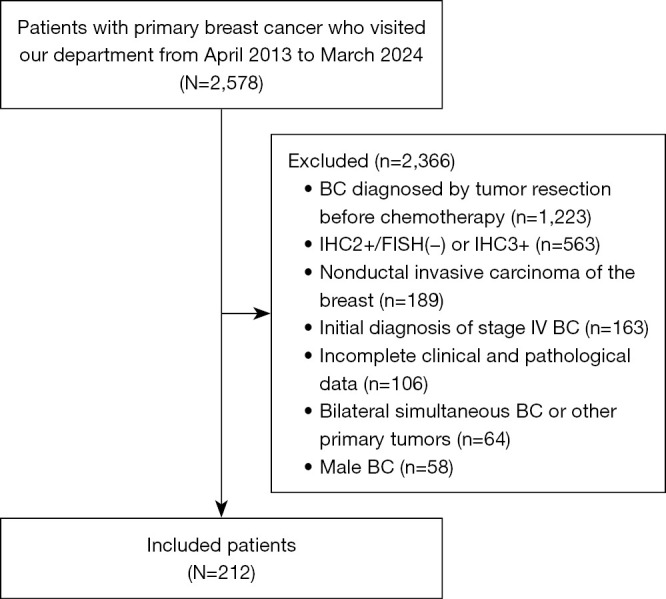
Methods: This study retrospectively included 212 patients with HER-2-low and HER-2-zero eBC treated with NAC and surgery from April 2013 to March 2024. The differences in the effects of NAC were compared at the imaging and pathological levels via Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and the Miller-Payne assessment criteria, and the clinical and core needle biopsy histopathological (CNB) features were analyzed to clarify the influencing factors. Moreover, the clinical and pathological factors influencing pCR after NAC for HER-2-low eBC were analyzed via univariate analysis and multifactorial binary logistic regression. A nomogram prediction model was constructed based on the independent influencing factors, diagnostic calibration curves were used for the goodness-of-fit test, and the performance of the prediction model was evaluated via receiver operating characteristic (ROC) curve analysis.
Results: HER-2-low eBC was associated with worse responsiveness to NAC at both the imaging and pathologic levels (P<0.05) and were significantly associated with estrogen receptor (ER)-positive status (P=0.03), progesterone receptor (PR)-positive status (P=0.04), and a low expression of Ki-67 (P=0.045). Univariate analysis indicated that a maximum tumor diameter >3 cm (P=0.04), positive axillary lymph nodes through puncture (P=0.001), fewer chemotherapeutic cycles (P=0.002), pathological grading I or II through puncture (P=0.04), ER-positive status (P=0.001), PR-positive status (P<0.001), low expression of Ki-67 (P=0.04), androgen receptor (AR)-positive status (P<0.001), and tumor invasion (P=0.002) were all unfavorable factors influencing pCR after NAC of HER-2-low eBC. Multifactorial analysis found that a maximum tumor diameter >3 cm [odds ratio (OR): 0.088; 95% confidence interval (CI): 0.015-0.529; P=0.008], positive axillary lymph nodes through puncture (OR: 18.677; 95% CI: 3.028-115.201; P=0.002), and fewer chemotherapeutic cycles (OR: 0.337; 95% CI: 0.148-0.764; P=0.009) were independent unfavorable factors. The area under the ROC of the nomogram prediction model for pCR after NAC for HER-2-low eBC was 0.861 (95% CI: 0.785-0.936), with a sensitivity of 80.0% and a specificity of 77.1%.
Conclusions: HER-2-low and HER-2-zero eBC respond differently to NAC and may need to be categorized in the future. Whether pCR can be achieved after NAC for HER-2-low eBC is influenced by multiple factors, and the nomogram prediction model has certain clinical prediction value.
期刊介绍:
Gland Surgery (Gland Surg; GS, Print ISSN 2227-684X; Online ISSN 2227-8575) being indexed by PubMed/PubMed Central, is an open access, peer-review journal launched at May of 2012, published bio-monthly since February 2015.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


