{"title":"迟发性髋关节发育不良的物理治疗管理:1例报告。","authors":"Kai-Yu Ho, Lisa Taylor, Katherine Joines","doi":"10.1155/crpe/5633998","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Delayed diagnosis of developmental dysplasia of the hip (DDH)-defined as detection after 8 weeks of age using physical examination, ultrasound, or X-ray-occurs in approximately 0.14%-0.26% of infants. This case report highlights the challenges of delayed DDH diagnosis and the role of physical therapy in rehabilitation. <b>Case Report:</b> The patient, a firstborn Asian female, was born vaginally at 40 weeks gestation. Her early medical history included left muscular torticollis, asymmetric crying faces syndrome, and laryngomalacia. Parents observed asymmetric gluteal folds, but early physical examinations before 3 months showed negative Barlow and Ortolani tests, normal hip range of motion, and no motor impairments. Thus, ultrasound imaging was not deemed necessary in early infancy due to negative physical exam findings, the absence of classic presentations and signs, and a lack of major risk factors that would typically warrant further imaging evaluation. At 11 months, signs of reduced weight bearing and leg length discrepancy led to radiographic evaluation, revealing left DDH with subluxation. Treatment included closed reduction, 14 weeks in a Spica cast, 14 months of abduction bracing, and physical therapy. Following casting, the patient experienced hip stiffness, limited mobility, and muscle weakness. Physical therapy focused on restoring movement while ensuring joint stability. With weekly sessions, the patient showed significant progress, achieving independent walking at 19 months. Follow-up radiographs demonstrated gradual acetabular index improvement, approaching normal development by age 6 years and 9 months. <b>Conclusion:</b> This case highlights the challenges of early DDH detection, the consequences of delayed diagnosis, and the vital role of physical therapy in postoperative recovery and functional development of children with DDH.</p>","PeriodicalId":9623,"journal":{"name":"Case Reports in Pediatrics","volume":"2025 ","pages":"5633998"},"PeriodicalIF":0.5000,"publicationDate":"2025-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425625/pdf/","citationCount":"0","resultStr":"{\"title\":\"Physical Therapy Management for Delayed Diagnosis of Developmental Dysplasia of the Hip: A Case Report.\",\"authors\":\"Kai-Yu Ho, Lisa Taylor, Katherine Joines\",\"doi\":\"10.1155/crpe/5633998\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Delayed diagnosis of developmental dysplasia of the hip (DDH)-defined as detection after 8 weeks of age using physical examination, ultrasound, or X-ray-occurs in approximately 0.14%-0.26% of infants. This case report highlights the challenges of delayed DDH diagnosis and the role of physical therapy in rehabilitation. <b>Case Report:</b> The patient, a firstborn Asian female, was born vaginally at 40 weeks gestation. Her early medical history included left muscular torticollis, asymmetric crying faces syndrome, and laryngomalacia. Parents observed asymmetric gluteal folds, but early physical examinations before 3 months showed negative Barlow and Ortolani tests, normal hip range of motion, and no motor impairments. Thus, ultrasound imaging was not deemed necessary in early infancy due to negative physical exam findings, the absence of classic presentations and signs, and a lack of major risk factors that would typically warrant further imaging evaluation. At 11 months, signs of reduced weight bearing and leg length discrepancy led to radiographic evaluation, revealing left DDH with subluxation. Treatment included closed reduction, 14 weeks in a Spica cast, 14 months of abduction bracing, and physical therapy. Following casting, the patient experienced hip stiffness, limited mobility, and muscle weakness. Physical therapy focused on restoring movement while ensuring joint stability. With weekly sessions, the patient showed significant progress, achieving independent walking at 19 months. Follow-up radiographs demonstrated gradual acetabular index improvement, approaching normal development by age 6 years and 9 months. <b>Conclusion:</b> This case highlights the challenges of early DDH detection, the consequences of delayed diagnosis, and the vital role of physical therapy in postoperative recovery and functional development of children with DDH.</p>\",\"PeriodicalId\":9623,\"journal\":{\"name\":\"Case Reports in Pediatrics\",\"volume\":\"2025 \",\"pages\":\"5633998\"},\"PeriodicalIF\":0.5000,\"publicationDate\":\"2025-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425625/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Pediatrics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crpe/5633998\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crpe/5633998","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
Physical Therapy Management for Delayed Diagnosis of Developmental Dysplasia of the Hip: A Case Report.
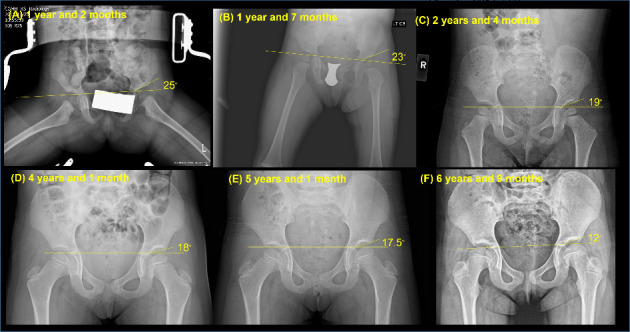
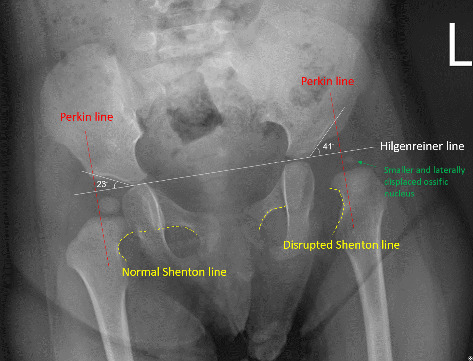
Background: Delayed diagnosis of developmental dysplasia of the hip (DDH)-defined as detection after 8 weeks of age using physical examination, ultrasound, or X-ray-occurs in approximately 0.14%-0.26% of infants. This case report highlights the challenges of delayed DDH diagnosis and the role of physical therapy in rehabilitation. Case Report: The patient, a firstborn Asian female, was born vaginally at 40 weeks gestation. Her early medical history included left muscular torticollis, asymmetric crying faces syndrome, and laryngomalacia. Parents observed asymmetric gluteal folds, but early physical examinations before 3 months showed negative Barlow and Ortolani tests, normal hip range of motion, and no motor impairments. Thus, ultrasound imaging was not deemed necessary in early infancy due to negative physical exam findings, the absence of classic presentations and signs, and a lack of major risk factors that would typically warrant further imaging evaluation. At 11 months, signs of reduced weight bearing and leg length discrepancy led to radiographic evaluation, revealing left DDH with subluxation. Treatment included closed reduction, 14 weeks in a Spica cast, 14 months of abduction bracing, and physical therapy. Following casting, the patient experienced hip stiffness, limited mobility, and muscle weakness. Physical therapy focused on restoring movement while ensuring joint stability. With weekly sessions, the patient showed significant progress, achieving independent walking at 19 months. Follow-up radiographs demonstrated gradual acetabular index improvement, approaching normal development by age 6 years and 9 months. Conclusion: This case highlights the challenges of early DDH detection, the consequences of delayed diagnosis, and the vital role of physical therapy in postoperative recovery and functional development of children with DDH.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


