Aleksi Raudasoja, Sameer Parpia, Jussi M J Mustonen, Robin Vernooij, Petra Falkenbach, Yoshitaka Aoki, Anton Barchuk, Marco H Blanker, Rufus Cartwright, Kathryn Crowder, Herney Andres Garcia-Perdomo, Rachel Gutschon, Alex L E Halme, Tuomas P Kilpeläinen, Ilari Kuitunen, Tiina Lamberg, Eddy Lang, Jenifer Matos, Olli P O Nevalainen, Niko K Nordlund, Negar Pourjamal, Eero Raittio, Patrick O Richard, Philippe D Violette, Jorma T Komulainen, Raija Sipilä, Kari A O Tikkinen
{"title":"初级保健中不同去实施策略的有效性:系统回顾和荟萃分析。","authors":"Aleksi Raudasoja, Sameer Parpia, Jussi M J Mustonen, Robin Vernooij, Petra Falkenbach, Yoshitaka Aoki, Anton Barchuk, Marco H Blanker, Rufus Cartwright, Kathryn Crowder, Herney Andres Garcia-Perdomo, Rachel Gutschon, Alex L E Halme, Tuomas P Kilpeläinen, Ilari Kuitunen, Tiina Lamberg, Eddy Lang, Jenifer Matos, Olli P O Nevalainen, Niko K Nordlund, Negar Pourjamal, Eero Raittio, Patrick O Richard, Philippe D Violette, Jorma T Komulainen, Raija Sipilä, Kari A O Tikkinen","doi":"10.1136/bmjmed-2025-001343","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the effectiveness of various de-implementation interventions in primary care, targeting care (treatments or tests) that provides no or limited value for patients (low value care).</p><p><strong>Design: </strong>Systematic review and meta-analysis.</p><p><strong>Data sources: </strong>Medline and Scopus databases, from inception to 10 July 2024.</p><p><strong>Eligibility criteria for selecting studies: </strong>Randomised trials comparing de-implementation interventions with placebo or sham intervention, no intervention, or other de-implementation intervention strategies in primary care. Eligible trials provided information on the use of low value care, total volume of care, appropriate care, and health outcomes.</p><p><strong>Data extraction and synthesis: </strong>Titles, abstracts, and full texts were screened, data were extracted, and risk of bias was assessed independently and in duplicate. Random effects meta-analyses were conducted, and the certainty of evidence was assessed with the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.</p><p><strong>Results: </strong>13 008 abstracts were screened and 140 were eligible for inclusion in the study. Median follow-up was 287 days (interquartile range 180-365). In 75 (54%) trials the aim was to reduce the use of antibiotics, in 42 (30%) to reduce other drug treatments, in 17 (12%) to reduce imaging, and in 15 (11%) to reduce laboratory testing. The certainty of the evidence was moderate that provider education combined with audit and feedback reduced the use of targeted low value care (odds ratio 0.73, 95% confidence interval (95% CI) 0.63 to 0.84). Provider education (0.86, 95% CI 0.72 to 1.03), audit and feedback (0.82, 0.67 to 1.00), and patient education (0.70, 0.30 to 1.66), and a combination of these strategies (point estimates for odds ratios ranging from 0.57 to 0.64) may reduce the use of targeted low value care (low certainty of evidence for all).</p><p><strong>Conclusions: </strong>The results suggested with moderate certainty of evidence that provider education combined with audit and feedback reduced the use of targeted low value care. Individual strategies may slightly reduce the use of targeted low value care, but achieving a meaningful impact on low value care may require the use of multiple strategies. The results may be useful for patients, clinicians, policy makers, and guideline developers when deciding on future de-implementation strategies and research priorities.</p><p><strong>Systematic review registration: </strong>PROSPERO CRD42023411768.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"4 1","pages":"e001343"},"PeriodicalIF":10.0000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421606/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of different de-implementation strategies in primary care: systematic review and meta-analysis.\",\"authors\":\"Aleksi Raudasoja, Sameer Parpia, Jussi M J Mustonen, Robin Vernooij, Petra Falkenbach, Yoshitaka Aoki, Anton Barchuk, Marco H Blanker, Rufus Cartwright, Kathryn Crowder, Herney Andres Garcia-Perdomo, Rachel Gutschon, Alex L E Halme, Tuomas P Kilpeläinen, Ilari Kuitunen, Tiina Lamberg, Eddy Lang, Jenifer Matos, Olli P O Nevalainen, Niko K Nordlund, Negar Pourjamal, Eero Raittio, Patrick O Richard, Philippe D Violette, Jorma T Komulainen, Raija Sipilä, Kari A O Tikkinen\",\"doi\":\"10.1136/bmjmed-2025-001343\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To evaluate the effectiveness of various de-implementation interventions in primary care, targeting care (treatments or tests) that provides no or limited value for patients (low value care).</p><p><strong>Design: </strong>Systematic review and meta-analysis.</p><p><strong>Data sources: </strong>Medline and Scopus databases, from inception to 10 July 2024.</p><p><strong>Eligibility criteria for selecting studies: </strong>Randomised trials comparing de-implementation interventions with placebo or sham intervention, no intervention, or other de-implementation intervention strategies in primary care. Eligible trials provided information on the use of low value care, total volume of care, appropriate care, and health outcomes.</p><p><strong>Data extraction and synthesis: </strong>Titles, abstracts, and full texts were screened, data were extracted, and risk of bias was assessed independently and in duplicate. Random effects meta-analyses were conducted, and the certainty of evidence was assessed with the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.</p><p><strong>Results: </strong>13 008 abstracts were screened and 140 were eligible for inclusion in the study. Median follow-up was 287 days (interquartile range 180-365). In 75 (54%) trials the aim was to reduce the use of antibiotics, in 42 (30%) to reduce other drug treatments, in 17 (12%) to reduce imaging, and in 15 (11%) to reduce laboratory testing. The certainty of the evidence was moderate that provider education combined with audit and feedback reduced the use of targeted low value care (odds ratio 0.73, 95% confidence interval (95% CI) 0.63 to 0.84). Provider education (0.86, 95% CI 0.72 to 1.03), audit and feedback (0.82, 0.67 to 1.00), and patient education (0.70, 0.30 to 1.66), and a combination of these strategies (point estimates for odds ratios ranging from 0.57 to 0.64) may reduce the use of targeted low value care (low certainty of evidence for all).</p><p><strong>Conclusions: </strong>The results suggested with moderate certainty of evidence that provider education combined with audit and feedback reduced the use of targeted low value care. Individual strategies may slightly reduce the use of targeted low value care, but achieving a meaningful impact on low value care may require the use of multiple strategies. The results may be useful for patients, clinicians, policy makers, and guideline developers when deciding on future de-implementation strategies and research priorities.</p><p><strong>Systematic review registration: </strong>PROSPERO CRD42023411768.</p>\",\"PeriodicalId\":72433,\"journal\":{\"name\":\"BMJ medicine\",\"volume\":\"4 1\",\"pages\":\"e001343\"},\"PeriodicalIF\":10.0000,\"publicationDate\":\"2025-09-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421606/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjmed-2025-001343\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2025-001343","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Effectiveness of different de-implementation strategies in primary care: systematic review and meta-analysis.
Objective: To evaluate the effectiveness of various de-implementation interventions in primary care, targeting care (treatments or tests) that provides no or limited value for patients (low value care).
Design: Systematic review and meta-analysis.
Data sources: Medline and Scopus databases, from inception to 10 July 2024.
Eligibility criteria for selecting studies: Randomised trials comparing de-implementation interventions with placebo or sham intervention, no intervention, or other de-implementation intervention strategies in primary care. Eligible trials provided information on the use of low value care, total volume of care, appropriate care, and health outcomes.
Data extraction and synthesis: Titles, abstracts, and full texts were screened, data were extracted, and risk of bias was assessed independently and in duplicate. Random effects meta-analyses were conducted, and the certainty of evidence was assessed with the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.
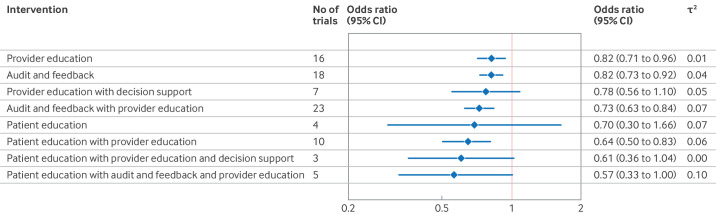
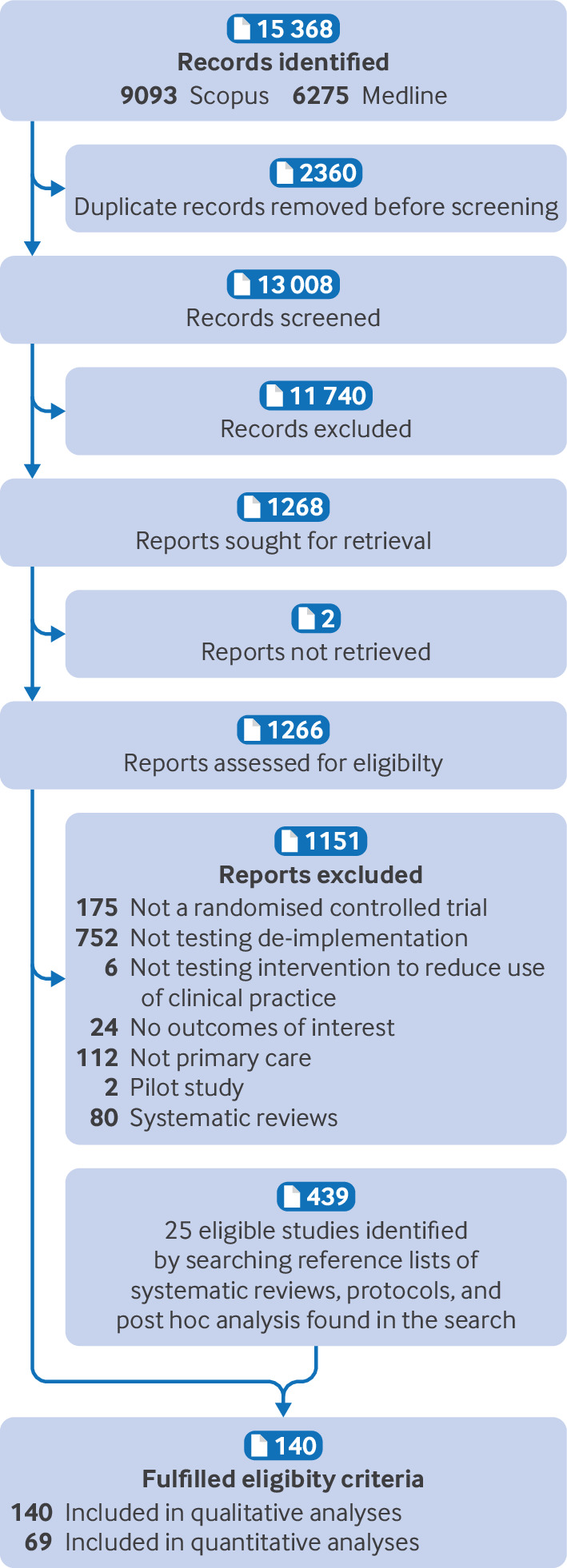
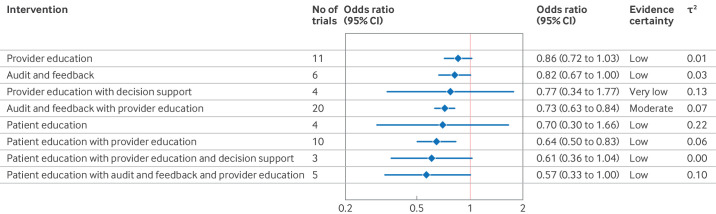
Results: 13 008 abstracts were screened and 140 were eligible for inclusion in the study. Median follow-up was 287 days (interquartile range 180-365). In 75 (54%) trials the aim was to reduce the use of antibiotics, in 42 (30%) to reduce other drug treatments, in 17 (12%) to reduce imaging, and in 15 (11%) to reduce laboratory testing. The certainty of the evidence was moderate that provider education combined with audit and feedback reduced the use of targeted low value care (odds ratio 0.73, 95% confidence interval (95% CI) 0.63 to 0.84). Provider education (0.86, 95% CI 0.72 to 1.03), audit and feedback (0.82, 0.67 to 1.00), and patient education (0.70, 0.30 to 1.66), and a combination of these strategies (point estimates for odds ratios ranging from 0.57 to 0.64) may reduce the use of targeted low value care (low certainty of evidence for all).
Conclusions: The results suggested with moderate certainty of evidence that provider education combined with audit and feedback reduced the use of targeted low value care. Individual strategies may slightly reduce the use of targeted low value care, but achieving a meaningful impact on low value care may require the use of multiple strategies. The results may be useful for patients, clinicians, policy makers, and guideline developers when deciding on future de-implementation strategies and research priorities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


