Yicong Chen, Yalin He, Xiaojuan Zhou, Ruixuan Yu, Yong Xu, Feng Peng, Bingwen Zou, Lin Zhou, Youling Gong, Jin Wang, Yongsheng Wang, Meijuan Huang, You Lu, Yongmei Liu
{"title":"提高晚期食管癌晚期免疫治疗的疗效:局部放疗的加入。","authors":"Yicong Chen, Yalin He, Xiaojuan Zhou, Ruixuan Yu, Yong Xu, Feng Peng, Bingwen Zou, Lin Zhou, Youling Gong, Jin Wang, Yongsheng Wang, Meijuan Huang, You Lu, Yongmei Liu","doi":"10.1177/17562848251371785","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The advent of immunotherapy has significantly revolutionized therapies for advanced esophageal cancer (EC). However, clinical data on combining immune checkpoint inhibitors (ICIs) and radiotherapy (RT) in advanced EC remain insufficient.</p><p><strong>Objectives: </strong>This study aimed to evaluate the effectiveness and safety of combining immunotherapy and radiation as a second or subsequent line of treatment for advanced EC.</p><p><strong>Design and methods: </strong>We retrospectively analyzed patients with advanced EC who received late-line ICIs and categorized them into two subgroups based on whether they received RT. The differences in survival and adverse events (AEs) were evaluated. Inverse probability of treatment weighting (IPTW) and 1:1 propensity-score matching (PSM) analysis were used to minimize confounding.</p><p><strong>Results: </strong>The analysis included data from 131 patients. The median progression-free survival (mPFS) was 9.1 months in the RT group, compared to 4.3 months in the non-radiotherapy (NRT) group (<i>p</i> = 0.0087). The median overall survival (mOS) was 13.5 months in the RT group, which is longer than the 7.3 months in the NRT group (<i>p</i> = 0.014). IPTW and 1:1 PSM analysis also showed that the RT group has longer mOS and mPFS. Among them, a higher biologically effective dose (BED) was associated with better survival than the lower dose group (16.1 months vs 10.2 months, <i>p</i> = 0.048). RT was an independent factor of better overall survival and progression-free survival in multivariable analysis, regardless of whether IPTW was used. For any grade of AE, any grade neutropenia (60.7% vs 41.4%, <i>p</i> = 0.028) and esophagitis (21.3% vs 1.4%, <i>p</i> < 0.001) were more common in the RT group. However, the incidence of grade 3-4 AEs did not differ significantly.</p><p><strong>Conclusion: </strong>Adding RT to second-line or later immunotherapy regimens for EC correlates with enhanced survival outcomes and manageable toxicity.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"18 ","pages":"17562848251371785"},"PeriodicalIF":3.4000,"publicationDate":"2025-09-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417674/pdf/","citationCount":"0","resultStr":"{\"title\":\"Improving the efficacy of late-line immunotherapy for advanced esophageal cancer: the addition of local radiotherapy.\",\"authors\":\"Yicong Chen, Yalin He, Xiaojuan Zhou, Ruixuan Yu, Yong Xu, Feng Peng, Bingwen Zou, Lin Zhou, Youling Gong, Jin Wang, Yongsheng Wang, Meijuan Huang, You Lu, Yongmei Liu\",\"doi\":\"10.1177/17562848251371785\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The advent of immunotherapy has significantly revolutionized therapies for advanced esophageal cancer (EC). However, clinical data on combining immune checkpoint inhibitors (ICIs) and radiotherapy (RT) in advanced EC remain insufficient.</p><p><strong>Objectives: </strong>This study aimed to evaluate the effectiveness and safety of combining immunotherapy and radiation as a second or subsequent line of treatment for advanced EC.</p><p><strong>Design and methods: </strong>We retrospectively analyzed patients with advanced EC who received late-line ICIs and categorized them into two subgroups based on whether they received RT. The differences in survival and adverse events (AEs) were evaluated. Inverse probability of treatment weighting (IPTW) and 1:1 propensity-score matching (PSM) analysis were used to minimize confounding.</p><p><strong>Results: </strong>The analysis included data from 131 patients. The median progression-free survival (mPFS) was 9.1 months in the RT group, compared to 4.3 months in the non-radiotherapy (NRT) group (<i>p</i> = 0.0087). The median overall survival (mOS) was 13.5 months in the RT group, which is longer than the 7.3 months in the NRT group (<i>p</i> = 0.014). IPTW and 1:1 PSM analysis also showed that the RT group has longer mOS and mPFS. Among them, a higher biologically effective dose (BED) was associated with better survival than the lower dose group (16.1 months vs 10.2 months, <i>p</i> = 0.048). RT was an independent factor of better overall survival and progression-free survival in multivariable analysis, regardless of whether IPTW was used. For any grade of AE, any grade neutropenia (60.7% vs 41.4%, <i>p</i> = 0.028) and esophagitis (21.3% vs 1.4%, <i>p</i> < 0.001) were more common in the RT group. However, the incidence of grade 3-4 AEs did not differ significantly.</p><p><strong>Conclusion: </strong>Adding RT to second-line or later immunotherapy regimens for EC correlates with enhanced survival outcomes and manageable toxicity.</p>\",\"PeriodicalId\":48770,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"18 \",\"pages\":\"17562848251371785\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-09-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417674/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848251371785\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848251371785","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:免疫疗法的出现极大地改变了晚期食管癌(EC)的治疗方法。然而,联合免疫检查点抑制剂(ICIs)和放疗(RT)治疗晚期EC的临床数据仍然不足。目的:本研究旨在评估免疫治疗和放疗联合作为晚期EC的二线或后续治疗的有效性和安全性。设计和方法:我们回顾性分析了接受晚期ICIs的晚期EC患者,并根据是否接受rt将其分为两个亚组。评估了生存和不良事件(ae)的差异。使用处理加权逆概率(IPTW)和1:1倾向评分匹配(PSM)分析来最大限度地减少混淆。结果:分析包括131例患者的数据。放疗组的中位无进展生存期(mPFS)为9.1个月,而非放疗组(NRT)为4.3个月(p = 0.0087)。RT组的中位总生存期(mOS)为13.5个月,高于NRT组的7.3个月(p = 0.014)。IPTW和1:1 PSM分析也显示RT组的mOS和mPFS更长。其中,较高的生物有效剂量(BED)与较低剂量组的生存率相关(16.1个月vs 10.2个月,p = 0.048)。在多变量分析中,无论是否使用IPTW, RT都是提高总生存期和无进展生存期的独立因素。对于任何级别的AE,任何级别的中性粒细胞减少(60.7% vs 41.4%, p = 0.028)和食管炎(21.3% vs 1.4%, p)结论:在二线或后期免疫治疗方案中添加RT与EC的生存结果和可控的毒性相关。
Improving the efficacy of late-line immunotherapy for advanced esophageal cancer: the addition of local radiotherapy.
Background: The advent of immunotherapy has significantly revolutionized therapies for advanced esophageal cancer (EC). However, clinical data on combining immune checkpoint inhibitors (ICIs) and radiotherapy (RT) in advanced EC remain insufficient.
Objectives: This study aimed to evaluate the effectiveness and safety of combining immunotherapy and radiation as a second or subsequent line of treatment for advanced EC.
Design and methods: We retrospectively analyzed patients with advanced EC who received late-line ICIs and categorized them into two subgroups based on whether they received RT. The differences in survival and adverse events (AEs) were evaluated. Inverse probability of treatment weighting (IPTW) and 1:1 propensity-score matching (PSM) analysis were used to minimize confounding.
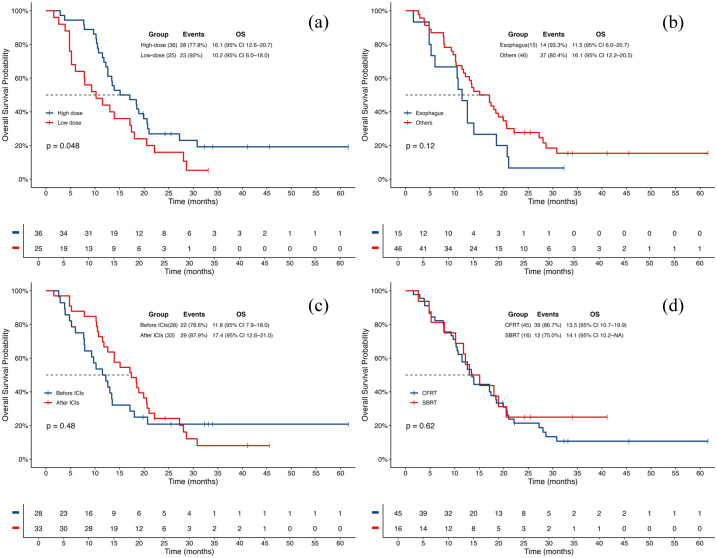
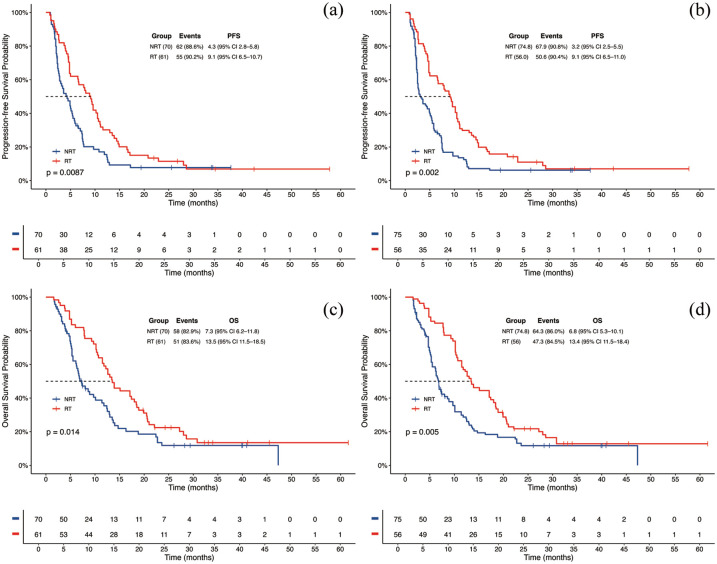
Results: The analysis included data from 131 patients. The median progression-free survival (mPFS) was 9.1 months in the RT group, compared to 4.3 months in the non-radiotherapy (NRT) group (p = 0.0087). The median overall survival (mOS) was 13.5 months in the RT group, which is longer than the 7.3 months in the NRT group (p = 0.014). IPTW and 1:1 PSM analysis also showed that the RT group has longer mOS and mPFS. Among them, a higher biologically effective dose (BED) was associated with better survival than the lower dose group (16.1 months vs 10.2 months, p = 0.048). RT was an independent factor of better overall survival and progression-free survival in multivariable analysis, regardless of whether IPTW was used. For any grade of AE, any grade neutropenia (60.7% vs 41.4%, p = 0.028) and esophagitis (21.3% vs 1.4%, p < 0.001) were more common in the RT group. However, the incidence of grade 3-4 AEs did not differ significantly.
Conclusion: Adding RT to second-line or later immunotherapy regimens for EC correlates with enhanced survival outcomes and manageable toxicity.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


