Xi Li, Bernhard P Berghout, Gijs van Rooijen, Mohammad Kamran Ikram, Bob Roozenbeek, Daniel Bos
{"title":"TIA或缺血性脑卒中患者的高血压、颅内动脉硬化和脑结构改变。","authors":"Xi Li, Bernhard P Berghout, Gijs van Rooijen, Mohammad Kamran Ikram, Bob Roozenbeek, Daniel Bos","doi":"10.1177/23969873241307099","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hypertension is a major risk factor of structural brain changes, including atrophy and cerebral small vessel disease. Intracranial arteriosclerosis could be an underlying mechanism between hypertension and structural brain changes. This study investigated whether intracranial carotid artery calcification (ICAC), as a proxy for intracranial arteriosclerosis, explains the association between hypertension and structural brain changes in patients with TIA or ischemic stroke.</p><p><strong>Patients and methods: </strong>About 968 patients (mean age 62.7 years) with TIA or ischemic stroke from a registry who underwent non-contrast CT (NCCT) and CT-angiography (CTA) were included in this study. Presence and volume (mm<sup>3</sup>) of ICAC were assessed on CTA. Subtypes of ICAC were assessed on NCCT, where ICAC was categorized into intimal and internal elastic lamina (IEL) type calcification. Structural brain changes, indicated by atrophy, periventricular and deep white matter lesions (WML), and lacunes were assessed on NCCT. Mediation analysis was performed using ICAC, ICAC volume, and ICAC subtypes as mediators.</p><p><strong>Results: </strong>ICAC was prevalent in 67.8% of patients, with 52.6% of them exhibiting intimal calcification, and 26.5% exhibiting IEL calcification. Atrophy, periventricular WML, deep WML, and lacunes were present in 48.1%, 56.4%, 43.0% and 17.1% of patients respectively. The presence of ICAC explained 7.1% of the association of hypertension with periventricular WML, 3.6% with deep WML, and 17.6% with lacunes. Hypertension was associated with increased atrophy through ICAC (OR: 1.02, 95% CI: 1.00-1.05). In subgroup analyses, IEL calcification partly explained the association between hypertension and periventricular WML (16.8%), and atrophy (OR: 1.12, 95% CI: 1.02-1.27). Intimal calcification did not explain any association.</p><p><strong>Conclusion: </strong>ICAC partially explained the association between hypertension and atrophy, periventricular and deep WML, and lacunes. Although intimal calcification was more prevalent in ischemic stroke patients, IEL calcification takes the leading role in explaining the association between hypertension and structural brain changes.</p>","PeriodicalId":46821,"journal":{"name":"European Stroke Journal","volume":"10 3","pages":"804-812"},"PeriodicalIF":4.5000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683788/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hypertension, intracranial arteriosclerosis, and structural brain changes in patients with TIA or ischemic stroke.\",\"authors\":\"Xi Li, Bernhard P Berghout, Gijs van Rooijen, Mohammad Kamran Ikram, Bob Roozenbeek, Daniel Bos\",\"doi\":\"10.1177/23969873241307099\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Hypertension is a major risk factor of structural brain changes, including atrophy and cerebral small vessel disease. Intracranial arteriosclerosis could be an underlying mechanism between hypertension and structural brain changes. This study investigated whether intracranial carotid artery calcification (ICAC), as a proxy for intracranial arteriosclerosis, explains the association between hypertension and structural brain changes in patients with TIA or ischemic stroke.</p><p><strong>Patients and methods: </strong>About 968 patients (mean age 62.7 years) with TIA or ischemic stroke from a registry who underwent non-contrast CT (NCCT) and CT-angiography (CTA) were included in this study. Presence and volume (mm<sup>3</sup>) of ICAC were assessed on CTA. Subtypes of ICAC were assessed on NCCT, where ICAC was categorized into intimal and internal elastic lamina (IEL) type calcification. Structural brain changes, indicated by atrophy, periventricular and deep white matter lesions (WML), and lacunes were assessed on NCCT. Mediation analysis was performed using ICAC, ICAC volume, and ICAC subtypes as mediators.</p><p><strong>Results: </strong>ICAC was prevalent in 67.8% of patients, with 52.6% of them exhibiting intimal calcification, and 26.5% exhibiting IEL calcification. Atrophy, periventricular WML, deep WML, and lacunes were present in 48.1%, 56.4%, 43.0% and 17.1% of patients respectively. The presence of ICAC explained 7.1% of the association of hypertension with periventricular WML, 3.6% with deep WML, and 17.6% with lacunes. Hypertension was associated with increased atrophy through ICAC (OR: 1.02, 95% CI: 1.00-1.05). In subgroup analyses, IEL calcification partly explained the association between hypertension and periventricular WML (16.8%), and atrophy (OR: 1.12, 95% CI: 1.02-1.27). Intimal calcification did not explain any association.</p><p><strong>Conclusion: </strong>ICAC partially explained the association between hypertension and atrophy, periventricular and deep WML, and lacunes. Although intimal calcification was more prevalent in ischemic stroke patients, IEL calcification takes the leading role in explaining the association between hypertension and structural brain changes.</p>\",\"PeriodicalId\":46821,\"journal\":{\"name\":\"European Stroke Journal\",\"volume\":\"10 3\",\"pages\":\"804-812\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683788/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Stroke Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/23969873241307099\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Stroke Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/23969873241307099","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Hypertension, intracranial arteriosclerosis, and structural brain changes in patients with TIA or ischemic stroke.
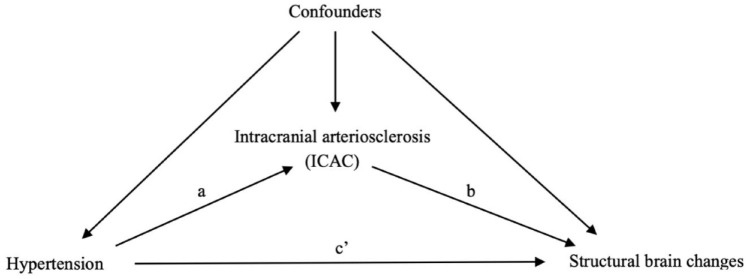
Introduction: Hypertension is a major risk factor of structural brain changes, including atrophy and cerebral small vessel disease. Intracranial arteriosclerosis could be an underlying mechanism between hypertension and structural brain changes. This study investigated whether intracranial carotid artery calcification (ICAC), as a proxy for intracranial arteriosclerosis, explains the association between hypertension and structural brain changes in patients with TIA or ischemic stroke.
Patients and methods: About 968 patients (mean age 62.7 years) with TIA or ischemic stroke from a registry who underwent non-contrast CT (NCCT) and CT-angiography (CTA) were included in this study. Presence and volume (mm3) of ICAC were assessed on CTA. Subtypes of ICAC were assessed on NCCT, where ICAC was categorized into intimal and internal elastic lamina (IEL) type calcification. Structural brain changes, indicated by atrophy, periventricular and deep white matter lesions (WML), and lacunes were assessed on NCCT. Mediation analysis was performed using ICAC, ICAC volume, and ICAC subtypes as mediators.
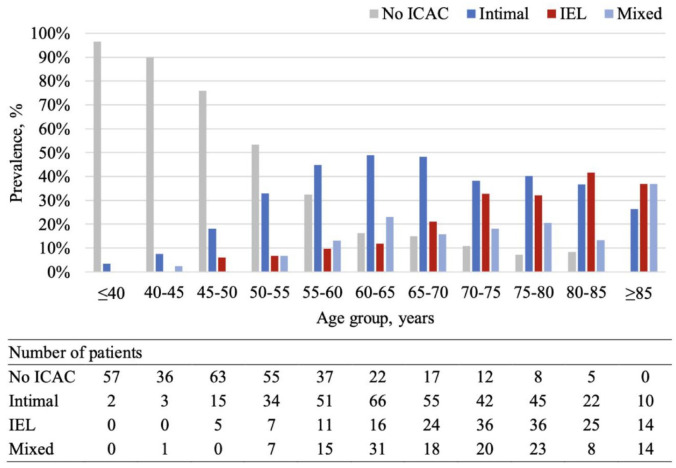
Results: ICAC was prevalent in 67.8% of patients, with 52.6% of them exhibiting intimal calcification, and 26.5% exhibiting IEL calcification. Atrophy, periventricular WML, deep WML, and lacunes were present in 48.1%, 56.4%, 43.0% and 17.1% of patients respectively. The presence of ICAC explained 7.1% of the association of hypertension with periventricular WML, 3.6% with deep WML, and 17.6% with lacunes. Hypertension was associated with increased atrophy through ICAC (OR: 1.02, 95% CI: 1.00-1.05). In subgroup analyses, IEL calcification partly explained the association between hypertension and periventricular WML (16.8%), and atrophy (OR: 1.12, 95% CI: 1.02-1.27). Intimal calcification did not explain any association.
Conclusion: ICAC partially explained the association between hypertension and atrophy, periventricular and deep WML, and lacunes. Although intimal calcification was more prevalent in ischemic stroke patients, IEL calcification takes the leading role in explaining the association between hypertension and structural brain changes.
期刊介绍:
Launched in 2016 the European Stroke Journal (ESJ) is the official journal of the European Stroke Organisation (ESO), a professional non-profit organization with over 1,400 individual members, and affiliations to numerous related national and international societies. ESJ covers clinical stroke research from all fields, including clinical trials, epidemiology, primary and secondary prevention, diagnosis, acute and post-acute management, guidelines, translation of experimental findings into clinical practice, rehabilitation, organisation of stroke care, and societal impact. It is open to authors from all relevant medical and health professions. Article types include review articles, original research, protocols, guidelines, editorials and letters to the Editor. Through ESJ, authors and researchers have gained a new platform for the rapid and professional publication of peer reviewed scientific material of the highest standards; publication in ESJ is highly competitive. The journal and its editorial team has developed excellent cooperation with sister organisations such as the World Stroke Organisation and the International Journal of Stroke, and the American Heart Organization/American Stroke Association and the journal Stroke. ESJ is fully peer-reviewed and is a member of the Committee on Publication Ethics (COPE). Issues are published 4 times a year (March, June, September and December) and articles are published OnlineFirst prior to issue publication.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


