{"title":"低剂量磺胺甲恶唑-甲氧苄啶可预防肾移植受者的肺囊虫肺炎:一项回顾性观察研究。","authors":"Rongrong Wang, Xiuhua Wu, Xishao Xie, Chunchun Wei, Jianyong Wu, Kuifen Ma","doi":"10.2147/TCRM.S528627","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Emerging evidence suggests that low doses of sulfamethoxazole-trimethoprim (TMP-SMX) may offer protection against <i>Pneumocystis jiroveci</i> pneumonia (PJP) in kidney transplant recipients. However, cases of PJP following the withdrawal of prophylaxis have been documented. This study aimed to investigate the relationship between the occurrence of PJP and different regimes of low-dose TMP-SMX prophylaxis.</p><p><strong>Methods: </strong>This retrospective observational study was conducted in the First Affiliated Hospital of Zhejiang University in China. Recipients diagnosed with PJP were included, and four controls were matched for each case based on transplantation time, age, and sex. Multivariate conditional logistic regression was employed to compare the odds of PJP occurrence among different TMP-SMX regimens.</p><p><strong>Results: </strong>From January 1, 2017, to December 31, 2020, 1763 patients underwent kidney transplantation at our center. Thirty-one patients developed PJP post-transplantation, and 124 patients without PJP were included as controls. One patient developed PJP during the prophylaxis period, and the others occurred after TMP-SMX discontinuation, resulting in a PJP incidence rate of 1.36% over the follow-up period. Compared to controls, the PJP group received a significantly lower cumulative TMP-SMX dose (median: 57 single-strength dose [SSD] tablets <i>vs</i> 100 tablets; <i>p = 0.001</i>) and had a shorter prophylaxis duration (median: 6.00 months <i>vs</i> 10.00 months; <i>p = 0.004</i>). They also exhibited higher CMV infection rates (29.0% vs 4.8%, <i>p</i> < 0.001), elevated serum creatinine levels at discharge (174.80μmol/L vs 134.58 μmol/L, <i>p</i> = 0.018), and reduced CD 4<sup>+</sup> cell counts (354.12/L vs 542.58/L, <i>p</i> = 0.05). Multivariate analysis revealed that a higher cumulative TMP-SMX dose was significantly associated with a lower risk of PJP (<i>p</i> = 0.005). Subgroup analysis indicated that at least 6 months of TMP-SMX prophylaxis is necessary for PJP prevention in recipients on quarter-strength daily (SMX/TMP 100/20 mg, <i>p</i> = 0.022) or half-single strength daily (SMX/TMP 200/40 to 400/80 mg, <i>p</i> = 0.005) regimens.</p><p><strong>Conclusion: </strong>An adequate prophylactic duration of either quarter-strength daily TMP-SMX or half-single strength daily TMP-SMX may protect kidney transplant recipients from PJP.</p>","PeriodicalId":22977,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"21 ","pages":"1333-1342"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422122/pdf/","citationCount":"0","resultStr":"{\"title\":\"Low-Dose Sulfamethoxazole-Trimethoprim Could Prevent <i>Pneumocystis jiroveci</i> Pneumonia in Kidney Transplant Recipients: A Retrospective, Observational Study.\",\"authors\":\"Rongrong Wang, Xiuhua Wu, Xishao Xie, Chunchun Wei, Jianyong Wu, Kuifen Ma\",\"doi\":\"10.2147/TCRM.S528627\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Emerging evidence suggests that low doses of sulfamethoxazole-trimethoprim (TMP-SMX) may offer protection against <i>Pneumocystis jiroveci</i> pneumonia (PJP) in kidney transplant recipients. However, cases of PJP following the withdrawal of prophylaxis have been documented. This study aimed to investigate the relationship between the occurrence of PJP and different regimes of low-dose TMP-SMX prophylaxis.</p><p><strong>Methods: </strong>This retrospective observational study was conducted in the First Affiliated Hospital of Zhejiang University in China. Recipients diagnosed with PJP were included, and four controls were matched for each case based on transplantation time, age, and sex. Multivariate conditional logistic regression was employed to compare the odds of PJP occurrence among different TMP-SMX regimens.</p><p><strong>Results: </strong>From January 1, 2017, to December 31, 2020, 1763 patients underwent kidney transplantation at our center. Thirty-one patients developed PJP post-transplantation, and 124 patients without PJP were included as controls. One patient developed PJP during the prophylaxis period, and the others occurred after TMP-SMX discontinuation, resulting in a PJP incidence rate of 1.36% over the follow-up period. Compared to controls, the PJP group received a significantly lower cumulative TMP-SMX dose (median: 57 single-strength dose [SSD] tablets <i>vs</i> 100 tablets; <i>p = 0.001</i>) and had a shorter prophylaxis duration (median: 6.00 months <i>vs</i> 10.00 months; <i>p = 0.004</i>). They also exhibited higher CMV infection rates (29.0% vs 4.8%, <i>p</i> < 0.001), elevated serum creatinine levels at discharge (174.80μmol/L vs 134.58 μmol/L, <i>p</i> = 0.018), and reduced CD 4<sup>+</sup> cell counts (354.12/L vs 542.58/L, <i>p</i> = 0.05). Multivariate analysis revealed that a higher cumulative TMP-SMX dose was significantly associated with a lower risk of PJP (<i>p</i> = 0.005). Subgroup analysis indicated that at least 6 months of TMP-SMX prophylaxis is necessary for PJP prevention in recipients on quarter-strength daily (SMX/TMP 100/20 mg, <i>p</i> = 0.022) or half-single strength daily (SMX/TMP 200/40 to 400/80 mg, <i>p</i> = 0.005) regimens.</p><p><strong>Conclusion: </strong>An adequate prophylactic duration of either quarter-strength daily TMP-SMX or half-single strength daily TMP-SMX may protect kidney transplant recipients from PJP.</p>\",\"PeriodicalId\":22977,\"journal\":{\"name\":\"Therapeutics and Clinical Risk Management\",\"volume\":\"21 \",\"pages\":\"1333-1342\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422122/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutics and Clinical Risk Management\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/TCRM.S528627\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"Pharmacology, Toxicology and Pharmaceutics\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S528627","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
引用次数: 0
摘要
目的:新出现的证据表明,低剂量磺胺甲恶唑-甲氧苄啶(TMP-SMX)可能对肾移植受者的肺囊虫肺炎(PJP)有保护作用。然而,在停止预防后出现PJP的病例已有记录。本研究旨在探讨不同低剂量TMP-SMX预防方案与PJP发生的关系。方法:回顾性观察研究在浙江大学第一附属医院进行。被诊断为PJP的受者包括在内,并根据移植时间、年龄和性别为每个病例匹配四名对照。采用多变量条件logistic回归比较不同TMP-SMX治疗方案中PJP发生的几率。结果:2017年1月1日至2020年12月31日,我院共收治肾移植患者1763例。31例移植后发生PJP, 124例未发生PJP的患者作为对照。1例患者在预防期间发生PJP,其余患者在停用TMP-SMX后发生,随访期间PJP发病率为1.36%。与对照组相比,PJP组接受的TMP-SMX累积剂量显著降低(中位数:57单剂量[SSD]片vs 100片;p = 0.001),预防持续时间更短(中位数:6.00个月vs 10.00个月;p = 0.004)。他们的CMV感染率也更高(29.0% vs 4.8%, p < 0.001),出院时血清肌酐水平升高(174.80μmol/L vs 134.58 μmol/L, p = 0.018), cd4 +细胞计数减少(354.12/L vs 542.58/L, p = 0.05)。多变量分析显示,较高的TMP-SMX累积剂量与较低的PJP风险显著相关(p = 0.005)。亚组分析表明,每日四分之一剂量(SMX/TMP 100/20 mg, p = 0.022)或每日半单一剂量(SMX/TMP 200/40至400/80 mg, p = 0.005)的患者预防PJP需要至少6个月的TMP-SMX预防。结论:适当的每日四分之一剂量TMP-SMX或每日半单剂量TMP-SMX的预防时间可以保护肾移植受者免受PJP的侵害。
Low-Dose Sulfamethoxazole-Trimethoprim Could Prevent Pneumocystis jiroveci Pneumonia in Kidney Transplant Recipients: A Retrospective, Observational Study.
Objective: Emerging evidence suggests that low doses of sulfamethoxazole-trimethoprim (TMP-SMX) may offer protection against Pneumocystis jiroveci pneumonia (PJP) in kidney transplant recipients. However, cases of PJP following the withdrawal of prophylaxis have been documented. This study aimed to investigate the relationship between the occurrence of PJP and different regimes of low-dose TMP-SMX prophylaxis.
Methods: This retrospective observational study was conducted in the First Affiliated Hospital of Zhejiang University in China. Recipients diagnosed with PJP were included, and four controls were matched for each case based on transplantation time, age, and sex. Multivariate conditional logistic regression was employed to compare the odds of PJP occurrence among different TMP-SMX regimens.
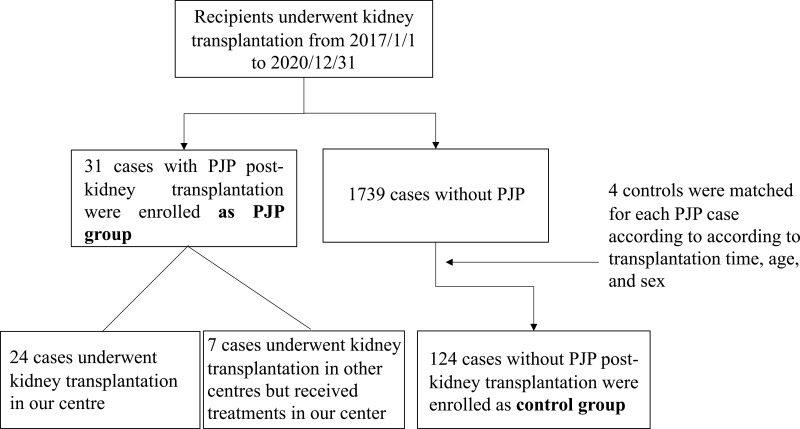
Results: From January 1, 2017, to December 31, 2020, 1763 patients underwent kidney transplantation at our center. Thirty-one patients developed PJP post-transplantation, and 124 patients without PJP were included as controls. One patient developed PJP during the prophylaxis period, and the others occurred after TMP-SMX discontinuation, resulting in a PJP incidence rate of 1.36% over the follow-up period. Compared to controls, the PJP group received a significantly lower cumulative TMP-SMX dose (median: 57 single-strength dose [SSD] tablets vs 100 tablets; p = 0.001) and had a shorter prophylaxis duration (median: 6.00 months vs 10.00 months; p = 0.004). They also exhibited higher CMV infection rates (29.0% vs 4.8%, p < 0.001), elevated serum creatinine levels at discharge (174.80μmol/L vs 134.58 μmol/L, p = 0.018), and reduced CD 4+ cell counts (354.12/L vs 542.58/L, p = 0.05). Multivariate analysis revealed that a higher cumulative TMP-SMX dose was significantly associated with a lower risk of PJP (p = 0.005). Subgroup analysis indicated that at least 6 months of TMP-SMX prophylaxis is necessary for PJP prevention in recipients on quarter-strength daily (SMX/TMP 100/20 mg, p = 0.022) or half-single strength daily (SMX/TMP 200/40 to 400/80 mg, p = 0.005) regimens.
Conclusion: An adequate prophylactic duration of either quarter-strength daily TMP-SMX or half-single strength daily TMP-SMX may protect kidney transplant recipients from PJP.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


