Vasavi Pushadapu, Srikanth Sriramozu, V Sahetya Mohan Rao, Sreekalyani Kothapally
{"title":"不良骨水泥的代价:一例慢性髋关节脱位及翻修。","authors":"Vasavi Pushadapu, Srikanth Sriramozu, V Sahetya Mohan Rao, Sreekalyani Kothapally","doi":"10.13107/jocr.2025.v15.i09.6092","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hemiarthroplasty is commonly performed for displaced femoral neck fractures in elderly patients. While generally effective, poor cementing techniques can lead to serious complications, including implant migration and chronic dislocation. Cement interposition in the acetabulum is a rare but preventable cause of persistent instability. This case emphasizes the importance of meticulous cement handling and intraoperative vigilance to avoid avoidable revision surgeries.</p><p><strong>Case report: </strong>A 76-year-old woman presented 8 months after left hemiarthroplasty with persistent hip pain and immobility. She had become bedridden 1-month post-surgery following a sensation of hip slippage. Examination revealed limb shortening, adduction deformity, and restricted mobility. Radiographs showed a dislocated hip and multiple dense opacities in the acetabulum, suggesting cement interposition. A posterior approach revision was planned. Pre-operative skin traction and adductor tenotomy were performed to address soft tissue contractures. Intraoperatively, well-formed cement mass conforming to the acetabulum was removed. The cement was removed en bloc, and a bipolar prosthesis was implanted. Post-operatively, the patient achieved satisfactory recovery with improved hip stability and function.</p><p><strong>Discussion: </strong>This case illustrates the potential for cement to migrate into the acetabulum during stem insertion if introduced pre-maturely or in excess. Such interposition disrupts joint articulation and can lead to chronic dislocation. Preventive steps - such as waiting for appropriate cement consistency, using a gauze barrier in the acetabulum, and careful intraoperative assessment - are critical to avoid such outcomes. Chronic dislocations further complicate surgical revisions due to soft tissue contractures and biomechanical imbalance. Comprehensive pre-operative planning and soft tissue management, combined with appropriate implant selection, contributed to successful revision in this case.</p><p><strong>Conclusion: </strong>Cement interposition is a rare but preventable cause of chronic dislocation after hemiarthroplasty. This case highlights the need for precise cementing techniques, careful intraoperative assessment, and proactive management strategies. Attention to these details can reduce complications and improve outcomes in elderly patients undergoing hip arthroplasty.</p>","PeriodicalId":16647,"journal":{"name":"Journal of Orthopaedic Case Reports","volume":"15 9","pages":"260-264"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422674/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Price of Poor Cementing: A Case Report on Chronic Hip Dislocation and Revision.\",\"authors\":\"Vasavi Pushadapu, Srikanth Sriramozu, V Sahetya Mohan Rao, Sreekalyani Kothapally\",\"doi\":\"10.13107/jocr.2025.v15.i09.6092\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Hemiarthroplasty is commonly performed for displaced femoral neck fractures in elderly patients. While generally effective, poor cementing techniques can lead to serious complications, including implant migration and chronic dislocation. Cement interposition in the acetabulum is a rare but preventable cause of persistent instability. This case emphasizes the importance of meticulous cement handling and intraoperative vigilance to avoid avoidable revision surgeries.</p><p><strong>Case report: </strong>A 76-year-old woman presented 8 months after left hemiarthroplasty with persistent hip pain and immobility. She had become bedridden 1-month post-surgery following a sensation of hip slippage. Examination revealed limb shortening, adduction deformity, and restricted mobility. Radiographs showed a dislocated hip and multiple dense opacities in the acetabulum, suggesting cement interposition. A posterior approach revision was planned. Pre-operative skin traction and adductor tenotomy were performed to address soft tissue contractures. Intraoperatively, well-formed cement mass conforming to the acetabulum was removed. The cement was removed en bloc, and a bipolar prosthesis was implanted. Post-operatively, the patient achieved satisfactory recovery with improved hip stability and function.</p><p><strong>Discussion: </strong>This case illustrates the potential for cement to migrate into the acetabulum during stem insertion if introduced pre-maturely or in excess. Such interposition disrupts joint articulation and can lead to chronic dislocation. Preventive steps - such as waiting for appropriate cement consistency, using a gauze barrier in the acetabulum, and careful intraoperative assessment - are critical to avoid such outcomes. Chronic dislocations further complicate surgical revisions due to soft tissue contractures and biomechanical imbalance. Comprehensive pre-operative planning and soft tissue management, combined with appropriate implant selection, contributed to successful revision in this case.</p><p><strong>Conclusion: </strong>Cement interposition is a rare but preventable cause of chronic dislocation after hemiarthroplasty. This case highlights the need for precise cementing techniques, careful intraoperative assessment, and proactive management strategies. Attention to these details can reduce complications and improve outcomes in elderly patients undergoing hip arthroplasty.</p>\",\"PeriodicalId\":16647,\"journal\":{\"name\":\"Journal of Orthopaedic Case Reports\",\"volume\":\"15 9\",\"pages\":\"260-264\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422674/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Orthopaedic Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.13107/jocr.2025.v15.i09.6092\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedic Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13107/jocr.2025.v15.i09.6092","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
The Price of Poor Cementing: A Case Report on Chronic Hip Dislocation and Revision.
Introduction: Hemiarthroplasty is commonly performed for displaced femoral neck fractures in elderly patients. While generally effective, poor cementing techniques can lead to serious complications, including implant migration and chronic dislocation. Cement interposition in the acetabulum is a rare but preventable cause of persistent instability. This case emphasizes the importance of meticulous cement handling and intraoperative vigilance to avoid avoidable revision surgeries.
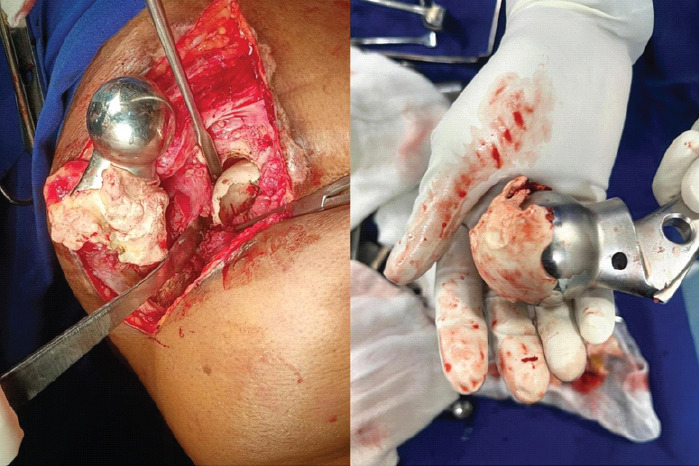
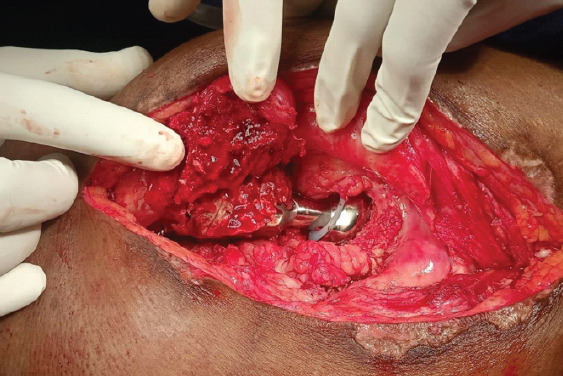
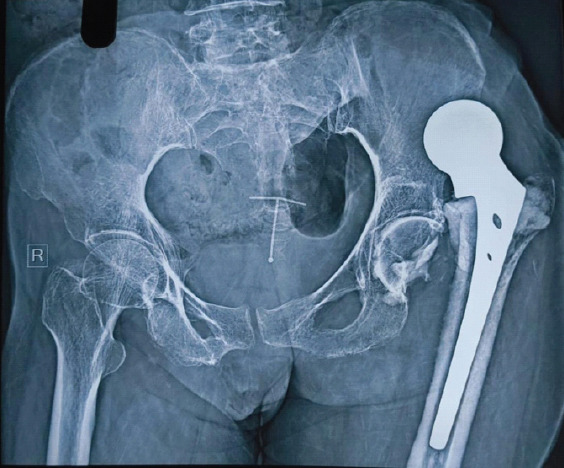
Case report: A 76-year-old woman presented 8 months after left hemiarthroplasty with persistent hip pain and immobility. She had become bedridden 1-month post-surgery following a sensation of hip slippage. Examination revealed limb shortening, adduction deformity, and restricted mobility. Radiographs showed a dislocated hip and multiple dense opacities in the acetabulum, suggesting cement interposition. A posterior approach revision was planned. Pre-operative skin traction and adductor tenotomy were performed to address soft tissue contractures. Intraoperatively, well-formed cement mass conforming to the acetabulum was removed. The cement was removed en bloc, and a bipolar prosthesis was implanted. Post-operatively, the patient achieved satisfactory recovery with improved hip stability and function.
Discussion: This case illustrates the potential for cement to migrate into the acetabulum during stem insertion if introduced pre-maturely or in excess. Such interposition disrupts joint articulation and can lead to chronic dislocation. Preventive steps - such as waiting for appropriate cement consistency, using a gauze barrier in the acetabulum, and careful intraoperative assessment - are critical to avoid such outcomes. Chronic dislocations further complicate surgical revisions due to soft tissue contractures and biomechanical imbalance. Comprehensive pre-operative planning and soft tissue management, combined with appropriate implant selection, contributed to successful revision in this case.
Conclusion: Cement interposition is a rare but preventable cause of chronic dislocation after hemiarthroplasty. This case highlights the need for precise cementing techniques, careful intraoperative assessment, and proactive management strategies. Attention to these details can reduce complications and improve outcomes in elderly patients undergoing hip arthroplasty.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


