{"title":"不可复位的前肩脱位合并大结节骨折:1例老年女性的操纵杆复位和二头肌保留。","authors":"Tao He","doi":"10.13107/jocr.2025.v15.i09.6060","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Low-energy traumatic irreducible anterior shoulder dislocations with concomitant greater tuberosity fractures in elderly females are rarely reported. The difficulty in reduction is attributed to the interplay between osseous impaction and soft tissue interposition. Three-dimensional computed tomography (CT) was utilized to delineate this combined obstruction mechanism. An open surgical approach incorporating joystick reduction techniques and preservation of the long head of the biceps tendon was implemented. To our knowledge, no systematic therapeutic protocols have been established for such complex injuries in geriatric patients.</p><p><strong>Case report: </strong>An 83-year-old Chinese female presented with left shoulder pain and restricted mobility after a ground-level fall. Physical examination revealed a squared shoulder deformity, deltoid muscle strength of 2/5, and sensory abnormalities in the axillary nerve territory. Radiographs confirmed anteroinferior humeral dislocation with comminuted greater tuberosity fracture. Closed reduction attempts failed twice. Three-dimensional.</p><p><strong>Ct demonstrated: </strong>① Hill-Sachs defect engaging the anterior glenoid rim; ② coronally split greater tuberosity fragment interposed in joint space; ③ 25 mm medial displacement of proximal humerus. The deltopectoral approach exposed the long head of biceps tendon traversing humeral head, forming complex interposition. Kirschner wire (K-wire) joystick technique was employed to disimpact osseous blocks. Tension band suturing combined with locking plate fixation was performed. Biceps tendon integrity was completely preserved. The post-operative course was uneventful, with satisfactory functional and radiographic outcomes and no recurrent dislocation during follow-up.</p><p><strong>Conclusion: </strong>This case demonstrates that three-dimensional CT precisely identifies osseous impaction mechanisms in irreducible anterior shoulder dislocations among elderly patients. Intraoperative K-wire joystick techniques combined with long head of biceps tendon preservation achieve anatomical reduction and stability restoration. This protocol establishes a standardized imaging-surgical framework for geriatric osteoporotic patients with failed closed reduction.</p>","PeriodicalId":16647,"journal":{"name":"Journal of Orthopaedic Case Reports","volume":"15 9","pages":"179-184"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422682/pdf/","citationCount":"0","resultStr":"{\"title\":\"Irreducible Anterior Shoulder Dislocation with Greater Tuberosity Fracture: Joystick Reduction and Biceps Preservation in an Elderly Female -A Case Report.\",\"authors\":\"Tao He\",\"doi\":\"10.13107/jocr.2025.v15.i09.6060\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Low-energy traumatic irreducible anterior shoulder dislocations with concomitant greater tuberosity fractures in elderly females are rarely reported. The difficulty in reduction is attributed to the interplay between osseous impaction and soft tissue interposition. Three-dimensional computed tomography (CT) was utilized to delineate this combined obstruction mechanism. An open surgical approach incorporating joystick reduction techniques and preservation of the long head of the biceps tendon was implemented. To our knowledge, no systematic therapeutic protocols have been established for such complex injuries in geriatric patients.</p><p><strong>Case report: </strong>An 83-year-old Chinese female presented with left shoulder pain and restricted mobility after a ground-level fall. Physical examination revealed a squared shoulder deformity, deltoid muscle strength of 2/5, and sensory abnormalities in the axillary nerve territory. Radiographs confirmed anteroinferior humeral dislocation with comminuted greater tuberosity fracture. Closed reduction attempts failed twice. Three-dimensional.</p><p><strong>Ct demonstrated: </strong>① Hill-Sachs defect engaging the anterior glenoid rim; ② coronally split greater tuberosity fragment interposed in joint space; ③ 25 mm medial displacement of proximal humerus. The deltopectoral approach exposed the long head of biceps tendon traversing humeral head, forming complex interposition. Kirschner wire (K-wire) joystick technique was employed to disimpact osseous blocks. Tension band suturing combined with locking plate fixation was performed. Biceps tendon integrity was completely preserved. The post-operative course was uneventful, with satisfactory functional and radiographic outcomes and no recurrent dislocation during follow-up.</p><p><strong>Conclusion: </strong>This case demonstrates that three-dimensional CT precisely identifies osseous impaction mechanisms in irreducible anterior shoulder dislocations among elderly patients. Intraoperative K-wire joystick techniques combined with long head of biceps tendon preservation achieve anatomical reduction and stability restoration. This protocol establishes a standardized imaging-surgical framework for geriatric osteoporotic patients with failed closed reduction.</p>\",\"PeriodicalId\":16647,\"journal\":{\"name\":\"Journal of Orthopaedic Case Reports\",\"volume\":\"15 9\",\"pages\":\"179-184\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422682/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Orthopaedic Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.13107/jocr.2025.v15.i09.6060\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedic Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13107/jocr.2025.v15.i09.6060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Irreducible Anterior Shoulder Dislocation with Greater Tuberosity Fracture: Joystick Reduction and Biceps Preservation in an Elderly Female -A Case Report.
Introduction: Low-energy traumatic irreducible anterior shoulder dislocations with concomitant greater tuberosity fractures in elderly females are rarely reported. The difficulty in reduction is attributed to the interplay between osseous impaction and soft tissue interposition. Three-dimensional computed tomography (CT) was utilized to delineate this combined obstruction mechanism. An open surgical approach incorporating joystick reduction techniques and preservation of the long head of the biceps tendon was implemented. To our knowledge, no systematic therapeutic protocols have been established for such complex injuries in geriatric patients.
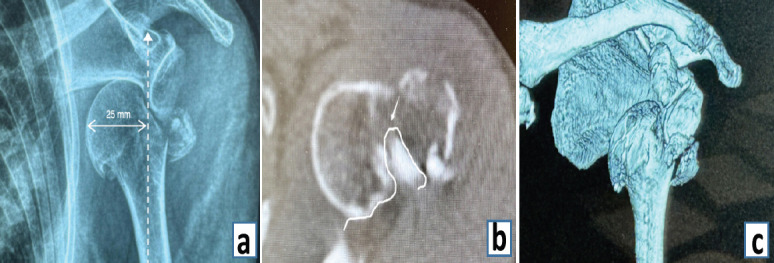
Case report: An 83-year-old Chinese female presented with left shoulder pain and restricted mobility after a ground-level fall. Physical examination revealed a squared shoulder deformity, deltoid muscle strength of 2/5, and sensory abnormalities in the axillary nerve territory. Radiographs confirmed anteroinferior humeral dislocation with comminuted greater tuberosity fracture. Closed reduction attempts failed twice. Three-dimensional.
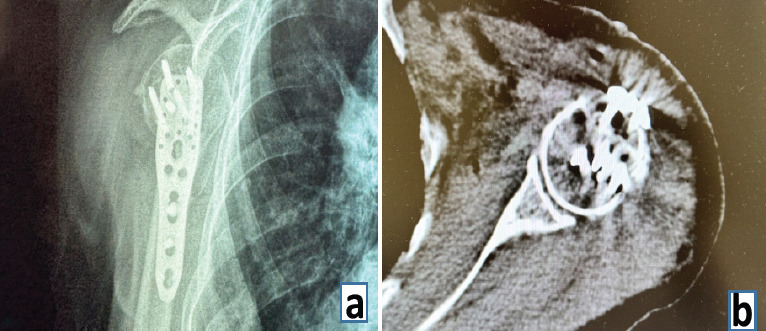
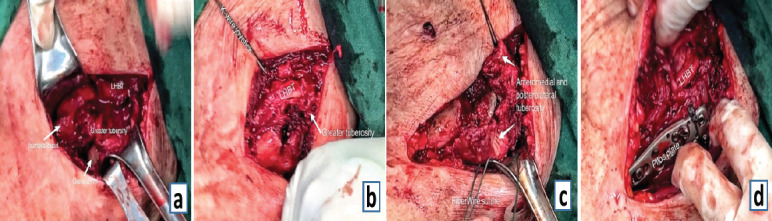
Ct demonstrated: ① Hill-Sachs defect engaging the anterior glenoid rim; ② coronally split greater tuberosity fragment interposed in joint space; ③ 25 mm medial displacement of proximal humerus. The deltopectoral approach exposed the long head of biceps tendon traversing humeral head, forming complex interposition. Kirschner wire (K-wire) joystick technique was employed to disimpact osseous blocks. Tension band suturing combined with locking plate fixation was performed. Biceps tendon integrity was completely preserved. The post-operative course was uneventful, with satisfactory functional and radiographic outcomes and no recurrent dislocation during follow-up.
Conclusion: This case demonstrates that three-dimensional CT precisely identifies osseous impaction mechanisms in irreducible anterior shoulder dislocations among elderly patients. Intraoperative K-wire joystick techniques combined with long head of biceps tendon preservation achieve anatomical reduction and stability restoration. This protocol establishes a standardized imaging-surgical framework for geriatric osteoporotic patients with failed closed reduction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


