Steve Fernandes, Santosh Jeevannavar, Keshav Shenoy, Prasanna Baindoor
{"title":"病理丰富的沉默肩:肩锁神经节囊肿的罕见表现。","authors":"Steve Fernandes, Santosh Jeevannavar, Keshav Shenoy, Prasanna Baindoor","doi":"10.13107/jocr.2025.v15.i09.6036","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The acromioclavicular (AC) ganglion cyst first described by a shoulder arthrogram by Craig in 1984, still remains an uncommon presentation of a shoulder pathology. Classified as a type one cyst by Hiller in the presence of a rotator cuff pathology, the management of these lesions is governed by ill-defined guidelines. Literature shows the variability of surgical management ranges from simple cyst excision and lateral end clavicular excision to reverse shoulder arthroplasty. Type two cysts are usually benign ganglion cysts, filled with mucinous putty material, and arise from the AC joint as a result of constant pressure of the synovial fluid passing in sequence, from the glenohumeral joint to the subacromial bursa and then reaching the AC joint. They are painless, gradually enlarging masses that appear just at the tip of the shoulder and, unless large, do not limit shoulder movements.</p><p><strong>Case report: </strong>We present to you a 77-year-old male patient with hypertension and diabetes, who came with a painless swelling over the right shoulder, gradually increasing in size for the first 6 months. He gave a prior history of pain in the shoulder associated with stiffness, depicting a frozen shoulder 5 years ago. On examination, the swelling was soft, cystic, non-reducible, fluctuant, measuring 3 × 3 cm centred over the AC joint. The range of motion was near normal, comparable to the opposite side, associated with crepitus, although pain free. Clinical special tests revealed intact but weak cuff muscles. Imaging was performed that revealed superior migration of the humeral head and near complete chronic supraspinatus tear with glenohumeral arthritis on radiograph. Magnetic resonance imaging showed synovial thickening with a cystic homogenous swelling above the AC joint, a cutoff geyser sign with no communication to the AC joint or subacromial bursa. Complete excision of the cyst in toto was performed with no additional procedure. The histopathological examination revealed a ganglion cyst.</p><p><strong>Conclusion: </strong>The AC joint cyst is a rare clinical diagnosis, requiring further insight into the spectrum of management of these lesions. In our case, the lack of clinical findings makes the management more challenging and thus, individualised.</p>","PeriodicalId":16647,"journal":{"name":"Journal of Orthopaedic Case Reports","volume":"15 9","pages":"116-120"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422636/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Silent Shoulder of Plentiful Pathology: An Uncommon Presentation of Acromioclavicular Ganglion Cyst.\",\"authors\":\"Steve Fernandes, Santosh Jeevannavar, Keshav Shenoy, Prasanna Baindoor\",\"doi\":\"10.13107/jocr.2025.v15.i09.6036\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The acromioclavicular (AC) ganglion cyst first described by a shoulder arthrogram by Craig in 1984, still remains an uncommon presentation of a shoulder pathology. Classified as a type one cyst by Hiller in the presence of a rotator cuff pathology, the management of these lesions is governed by ill-defined guidelines. Literature shows the variability of surgical management ranges from simple cyst excision and lateral end clavicular excision to reverse shoulder arthroplasty. Type two cysts are usually benign ganglion cysts, filled with mucinous putty material, and arise from the AC joint as a result of constant pressure of the synovial fluid passing in sequence, from the glenohumeral joint to the subacromial bursa and then reaching the AC joint. They are painless, gradually enlarging masses that appear just at the tip of the shoulder and, unless large, do not limit shoulder movements.</p><p><strong>Case report: </strong>We present to you a 77-year-old male patient with hypertension and diabetes, who came with a painless swelling over the right shoulder, gradually increasing in size for the first 6 months. He gave a prior history of pain in the shoulder associated with stiffness, depicting a frozen shoulder 5 years ago. On examination, the swelling was soft, cystic, non-reducible, fluctuant, measuring 3 × 3 cm centred over the AC joint. The range of motion was near normal, comparable to the opposite side, associated with crepitus, although pain free. Clinical special tests revealed intact but weak cuff muscles. Imaging was performed that revealed superior migration of the humeral head and near complete chronic supraspinatus tear with glenohumeral arthritis on radiograph. Magnetic resonance imaging showed synovial thickening with a cystic homogenous swelling above the AC joint, a cutoff geyser sign with no communication to the AC joint or subacromial bursa. Complete excision of the cyst in toto was performed with no additional procedure. The histopathological examination revealed a ganglion cyst.</p><p><strong>Conclusion: </strong>The AC joint cyst is a rare clinical diagnosis, requiring further insight into the spectrum of management of these lesions. In our case, the lack of clinical findings makes the management more challenging and thus, individualised.</p>\",\"PeriodicalId\":16647,\"journal\":{\"name\":\"Journal of Orthopaedic Case Reports\",\"volume\":\"15 9\",\"pages\":\"116-120\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422636/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Orthopaedic Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.13107/jocr.2025.v15.i09.6036\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedic Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13107/jocr.2025.v15.i09.6036","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A Silent Shoulder of Plentiful Pathology: An Uncommon Presentation of Acromioclavicular Ganglion Cyst.
Introduction: The acromioclavicular (AC) ganglion cyst first described by a shoulder arthrogram by Craig in 1984, still remains an uncommon presentation of a shoulder pathology. Classified as a type one cyst by Hiller in the presence of a rotator cuff pathology, the management of these lesions is governed by ill-defined guidelines. Literature shows the variability of surgical management ranges from simple cyst excision and lateral end clavicular excision to reverse shoulder arthroplasty. Type two cysts are usually benign ganglion cysts, filled with mucinous putty material, and arise from the AC joint as a result of constant pressure of the synovial fluid passing in sequence, from the glenohumeral joint to the subacromial bursa and then reaching the AC joint. They are painless, gradually enlarging masses that appear just at the tip of the shoulder and, unless large, do not limit shoulder movements.
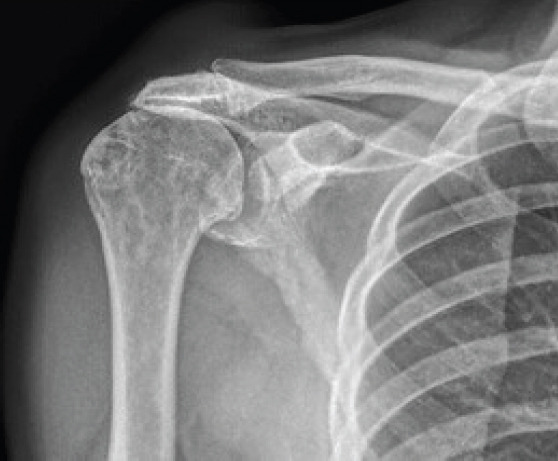
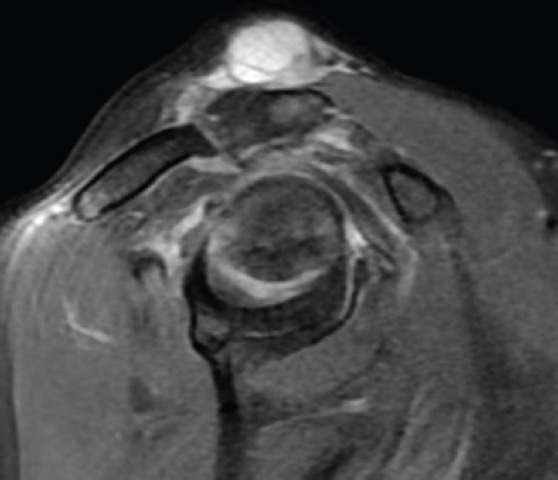
Case report: We present to you a 77-year-old male patient with hypertension and diabetes, who came with a painless swelling over the right shoulder, gradually increasing in size for the first 6 months. He gave a prior history of pain in the shoulder associated with stiffness, depicting a frozen shoulder 5 years ago. On examination, the swelling was soft, cystic, non-reducible, fluctuant, measuring 3 × 3 cm centred over the AC joint. The range of motion was near normal, comparable to the opposite side, associated with crepitus, although pain free. Clinical special tests revealed intact but weak cuff muscles. Imaging was performed that revealed superior migration of the humeral head and near complete chronic supraspinatus tear with glenohumeral arthritis on radiograph. Magnetic resonance imaging showed synovial thickening with a cystic homogenous swelling above the AC joint, a cutoff geyser sign with no communication to the AC joint or subacromial bursa. Complete excision of the cyst in toto was performed with no additional procedure. The histopathological examination revealed a ganglion cyst.
Conclusion: The AC joint cyst is a rare clinical diagnosis, requiring further insight into the spectrum of management of these lesions. In our case, the lack of clinical findings makes the management more challenging and thus, individualised.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


