Bolu Yang, Enying Gong, Xingxing Chen, Jie Tan, Nicholas Peoples, Yuhan Li, Jiayu Cai, Yan Li, Brian Oldenburg, Chen Chen, Dejin Dong, Xiaochen Zhang, Eric Finkelstein, Lei Si, Lijing L Yan
{"title":"中国农村卒中管理多组分移动健康干预的经济评价:6年随访的集群随机试验","authors":"Bolu Yang, Enying Gong, Xingxing Chen, Jie Tan, Nicholas Peoples, Yuhan Li, Jiayu Cai, Yan Li, Brian Oldenburg, Chen Chen, Dejin Dong, Xiaochen Zhang, Eric Finkelstein, Lei Si, Lijing L Yan","doi":"10.2196/75326","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To bridge the gap between clinical guidelines and suboptimal stroke management in rural settings, we conducted an implementation trial using evidence-based, mobile health-enabled strategies to empower primary care providers in rural China. The system-integrated and digital technology-enabled model of care (SINEMA) model was shown to significantly reduce blood pressure and mortality among people with stroke in rural China.</p><p><strong>Objective: </strong>This study aimed to evaluate the cost-effectiveness of the SINEMA intervention within both the active trial and the post-trial observational periods and its budget impact for potential nationwide scalability.</p><p><strong>Methods: </strong>In the cluster-randomized implementation trial (the SINEMA trial), 50 villages were randomized to either a 1-year intervention (2017-2018) or usual care, with 1299 patients with stroke followed up until 2022-2023-6 years after the trial baseline. The incremental cost-effectiveness ratios (ICER) for systolic blood pressure reduction and quality-adjusted life year gains were estimated from a health sector perspective. Both probabilistic and deterministic sensitivity analyses were conducted to assess the robustness of the findings. Additionally, a budget impact analysis was performed from a public payer perspective to estimate the per-capita and total costs of national scale-up under 2 scenarios: a standalone intervention and integration into the existing basic public health service system.</p><p><strong>Results: </strong>The ICER per 1 mmHg systolic blood pressure reduction was $8.4 for the within-trial estimation. The ICER per quality-adjusted life year gained was $837.9 within-trial and $727.9 post-trial, both highly cost-effective relative to any commonly adopted thresholds and robust in sensitivity analyses. The first-year budget impact ranged from $115.6 million to $197.7 million in the 2 scenarios, reducing to $46.6 million to $78.7 million by year 5, with a per-capita cost of $0.03-$0.06.</p><p><strong>Conclusions: </strong>Our findings demonstrate that the SINEMA intervention was cost-effective during the trial period and remained so throughout the 6-year sustainability observation period. These results highlight the potential of adopting similar health system-integrated, mobile health-enabled strategies to enhance the management of stroke and other chronic diseases in resource-limited settings.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT0318585, ClinicalTrials.gov NCT05792618; https://clinicaltrials.gov/study/NCT03185858 and https://clinicaltrials.gov/study/NCT05792618.</p><p><strong>International registered report identifier (irrid): </strong>RR2-10.3389/fneur.2023.1145562.</p>","PeriodicalId":14756,"journal":{"name":"JMIR mHealth and uHealth","volume":"13 ","pages":"e75326"},"PeriodicalIF":6.2000,"publicationDate":"2025-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12464504/pdf/","citationCount":"0","resultStr":"{\"title\":\"Economic Evaluation of a Multicomponent mHealth Intervention for Stroke Management in Rural China: Cluster-Randomized Trial With 6-Year Follow-Up.\",\"authors\":\"Bolu Yang, Enying Gong, Xingxing Chen, Jie Tan, Nicholas Peoples, Yuhan Li, Jiayu Cai, Yan Li, Brian Oldenburg, Chen Chen, Dejin Dong, Xiaochen Zhang, Eric Finkelstein, Lei Si, Lijing L Yan\",\"doi\":\"10.2196/75326\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>To bridge the gap between clinical guidelines and suboptimal stroke management in rural settings, we conducted an implementation trial using evidence-based, mobile health-enabled strategies to empower primary care providers in rural China. The system-integrated and digital technology-enabled model of care (SINEMA) model was shown to significantly reduce blood pressure and mortality among people with stroke in rural China.</p><p><strong>Objective: </strong>This study aimed to evaluate the cost-effectiveness of the SINEMA intervention within both the active trial and the post-trial observational periods and its budget impact for potential nationwide scalability.</p><p><strong>Methods: </strong>In the cluster-randomized implementation trial (the SINEMA trial), 50 villages were randomized to either a 1-year intervention (2017-2018) or usual care, with 1299 patients with stroke followed up until 2022-2023-6 years after the trial baseline. The incremental cost-effectiveness ratios (ICER) for systolic blood pressure reduction and quality-adjusted life year gains were estimated from a health sector perspective. Both probabilistic and deterministic sensitivity analyses were conducted to assess the robustness of the findings. Additionally, a budget impact analysis was performed from a public payer perspective to estimate the per-capita and total costs of national scale-up under 2 scenarios: a standalone intervention and integration into the existing basic public health service system.</p><p><strong>Results: </strong>The ICER per 1 mmHg systolic blood pressure reduction was $8.4 for the within-trial estimation. The ICER per quality-adjusted life year gained was $837.9 within-trial and $727.9 post-trial, both highly cost-effective relative to any commonly adopted thresholds and robust in sensitivity analyses. The first-year budget impact ranged from $115.6 million to $197.7 million in the 2 scenarios, reducing to $46.6 million to $78.7 million by year 5, with a per-capita cost of $0.03-$0.06.</p><p><strong>Conclusions: </strong>Our findings demonstrate that the SINEMA intervention was cost-effective during the trial period and remained so throughout the 6-year sustainability observation period. These results highlight the potential of adopting similar health system-integrated, mobile health-enabled strategies to enhance the management of stroke and other chronic diseases in resource-limited settings.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT0318585, ClinicalTrials.gov NCT05792618; https://clinicaltrials.gov/study/NCT03185858 and https://clinicaltrials.gov/study/NCT05792618.</p><p><strong>International registered report identifier (irrid): </strong>RR2-10.3389/fneur.2023.1145562.</p>\",\"PeriodicalId\":14756,\"journal\":{\"name\":\"JMIR mHealth and uHealth\",\"volume\":\"13 \",\"pages\":\"e75326\"},\"PeriodicalIF\":6.2000,\"publicationDate\":\"2025-09-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12464504/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR mHealth and uHealth\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2196/75326\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR mHealth and uHealth","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2196/75326","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Economic Evaluation of a Multicomponent mHealth Intervention for Stroke Management in Rural China: Cluster-Randomized Trial With 6-Year Follow-Up.
Background: To bridge the gap between clinical guidelines and suboptimal stroke management in rural settings, we conducted an implementation trial using evidence-based, mobile health-enabled strategies to empower primary care providers in rural China. The system-integrated and digital technology-enabled model of care (SINEMA) model was shown to significantly reduce blood pressure and mortality among people with stroke in rural China.
Objective: This study aimed to evaluate the cost-effectiveness of the SINEMA intervention within both the active trial and the post-trial observational periods and its budget impact for potential nationwide scalability.
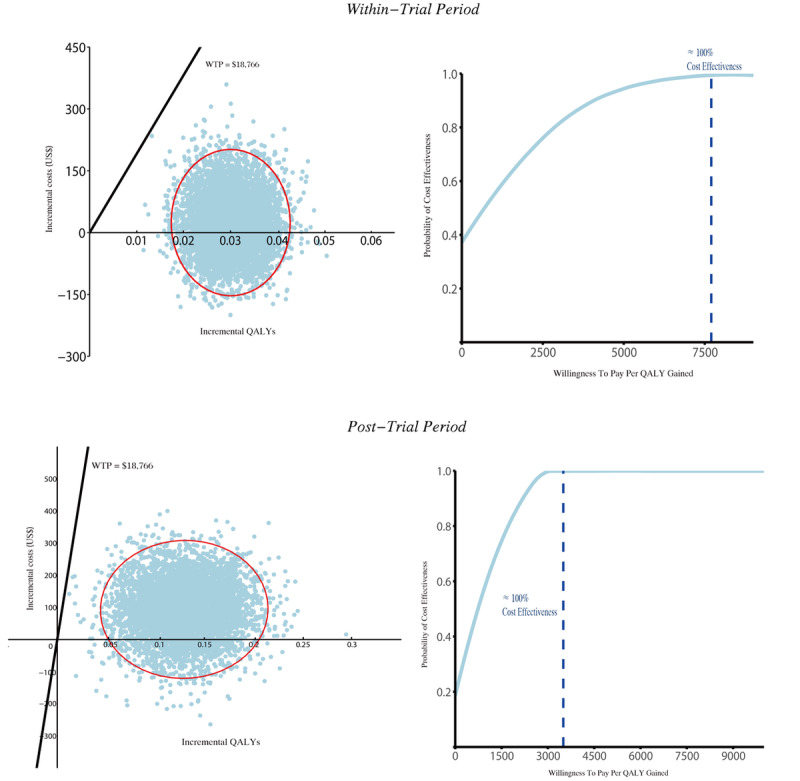
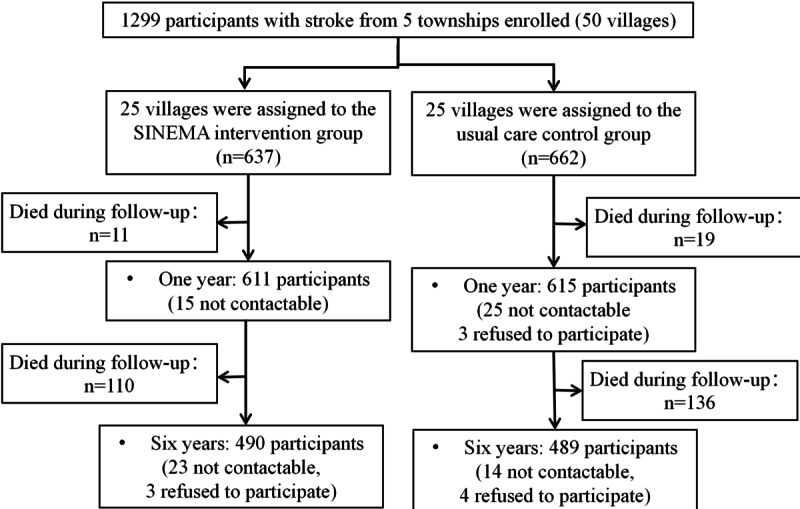
Methods: In the cluster-randomized implementation trial (the SINEMA trial), 50 villages were randomized to either a 1-year intervention (2017-2018) or usual care, with 1299 patients with stroke followed up until 2022-2023-6 years after the trial baseline. The incremental cost-effectiveness ratios (ICER) for systolic blood pressure reduction and quality-adjusted life year gains were estimated from a health sector perspective. Both probabilistic and deterministic sensitivity analyses were conducted to assess the robustness of the findings. Additionally, a budget impact analysis was performed from a public payer perspective to estimate the per-capita and total costs of national scale-up under 2 scenarios: a standalone intervention and integration into the existing basic public health service system.
Results: The ICER per 1 mmHg systolic blood pressure reduction was $8.4 for the within-trial estimation. The ICER per quality-adjusted life year gained was $837.9 within-trial and $727.9 post-trial, both highly cost-effective relative to any commonly adopted thresholds and robust in sensitivity analyses. The first-year budget impact ranged from $115.6 million to $197.7 million in the 2 scenarios, reducing to $46.6 million to $78.7 million by year 5, with a per-capita cost of $0.03-$0.06.
Conclusions: Our findings demonstrate that the SINEMA intervention was cost-effective during the trial period and remained so throughout the 6-year sustainability observation period. These results highlight the potential of adopting similar health system-integrated, mobile health-enabled strategies to enhance the management of stroke and other chronic diseases in resource-limited settings.
Trial registration: ClinicalTrials.gov NCT0318585, ClinicalTrials.gov NCT05792618; https://clinicaltrials.gov/study/NCT03185858 and https://clinicaltrials.gov/study/NCT05792618.
International registered report identifier (irrid): RR2-10.3389/fneur.2023.1145562.
期刊介绍:
JMIR mHealth and uHealth (JMU, ISSN 2291-5222) is a spin-off journal of JMIR, the leading eHealth journal (Impact Factor 2016: 5.175). JMIR mHealth and uHealth is indexed in PubMed, PubMed Central, and Science Citation Index Expanded (SCIE), and in June 2017 received a stunning inaugural Impact Factor of 4.636.
The journal focusses on health and biomedical applications in mobile and tablet computing, pervasive and ubiquitous computing, wearable computing and domotics.
JMIR mHealth and uHealth publishes since 2013 and was the first mhealth journal in Pubmed. It publishes even faster and has a broader scope with including papers which are more technical or more formative/developmental than what would be published in the Journal of Medical Internet Research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


