Aipi Forsberg-Puckett, Gabriele Wurm Johansson, Sara Regnér
{"title":"一项连续回顾性队列研究显示,接受抗栓治疗的患者出现胃肠道出血。","authors":"Aipi Forsberg-Puckett, Gabriele Wurm Johansson, Sara Regnér","doi":"10.1186/s13049-025-01431-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antithrombotic treatment might affect bleeding symptoms, identification of bleeding source and treatment for patients with acute gastrointestinal bleeding. This study aims to investigate possible differences in initial bleeding symptoms, identified bleeding site and treatment of patients with or without antithrombotic medication admitted for gastrointestinal bleeding.</p><p><strong>Methods: </strong>All consecutive adult patients primarily admitted for gastrointestinal bleeding at Skane University Hospital between 2018-01-01 and 2019-06-31, were included in this study. Data was retrospectively extracted from medical files. Patients were stratified according to antithrombotic therapy (antiplatelet or oral anticoagulants) on admittance or not. Groups were compared using Fisher's exact test, Mann Whitney U-test, Kruskal-Wallis test and logistic regression analysis, including interaction models.</p><p><strong>Results: </strong>585 patients were included. Median age was 75 years and a majority (58%) were male. In total, 269 (46%) patients had no antithrombotic medication and 316 (54%) had some kind of antithrombotic medication. Patients with antithrombotic therapy had a higher age and Charlson comorbidity index than those without antithrombotic therapy. However, comparing patients with anticoagulants, antiplatelet medication and no antithrombotics, hemoglobin at arrival (median (interquartile range (IQR)) 99(75-130), 103(85-125) and 100(80-128) respectively, p = 0.851) and Shock index (0.65 (0.50-0.83), 0.67(0.53-0.81) and 0.66 (0.57-0.80) respectively, p = 0.529) did not differ between the groups. Patients with antithrombotic therapy more often presented with hematochezia alone (35.3% and 32.2% for anticoagulant and antiplatelet medications, respectively, 23% for those with no antithrombotics p = 0.017) and less frequently with hematemesis compared to patients with no antithrombotic therapy (14.7% and 24.6%, respectively, 33.1% in those with no antithrombotics, p < 0.001). Predicted probabilities of receiving endoscopic treatment, need for transfusion, and number of units transfused did not differ between groups.</p><p><strong>Conclusions: </strong>Patients with anticoagulant therapy more often present with a lower source of Gastrointestinal (GI) bleeding than both those on antiplatelet medications and those with no antithrombotics. However, the presentation of bleeding is similar regardless of any antithrombotic medication or not.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov (NCT05195697), 19/01/2022.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"146"},"PeriodicalIF":3.1000,"publicationDate":"2025-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421751/pdf/","citationCount":"0","resultStr":"{\"title\":\"Presentation of gastrointestinal bleeding in patients with antithrombotic therapy, results from a consecutive retrospective cohort.\",\"authors\":\"Aipi Forsberg-Puckett, Gabriele Wurm Johansson, Sara Regnér\",\"doi\":\"10.1186/s13049-025-01431-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Antithrombotic treatment might affect bleeding symptoms, identification of bleeding source and treatment for patients with acute gastrointestinal bleeding. This study aims to investigate possible differences in initial bleeding symptoms, identified bleeding site and treatment of patients with or without antithrombotic medication admitted for gastrointestinal bleeding.</p><p><strong>Methods: </strong>All consecutive adult patients primarily admitted for gastrointestinal bleeding at Skane University Hospital between 2018-01-01 and 2019-06-31, were included in this study. Data was retrospectively extracted from medical files. Patients were stratified according to antithrombotic therapy (antiplatelet or oral anticoagulants) on admittance or not. Groups were compared using Fisher's exact test, Mann Whitney U-test, Kruskal-Wallis test and logistic regression analysis, including interaction models.</p><p><strong>Results: </strong>585 patients were included. Median age was 75 years and a majority (58%) were male. In total, 269 (46%) patients had no antithrombotic medication and 316 (54%) had some kind of antithrombotic medication. Patients with antithrombotic therapy had a higher age and Charlson comorbidity index than those without antithrombotic therapy. However, comparing patients with anticoagulants, antiplatelet medication and no antithrombotics, hemoglobin at arrival (median (interquartile range (IQR)) 99(75-130), 103(85-125) and 100(80-128) respectively, p = 0.851) and Shock index (0.65 (0.50-0.83), 0.67(0.53-0.81) and 0.66 (0.57-0.80) respectively, p = 0.529) did not differ between the groups. Patients with antithrombotic therapy more often presented with hematochezia alone (35.3% and 32.2% for anticoagulant and antiplatelet medications, respectively, 23% for those with no antithrombotics p = 0.017) and less frequently with hematemesis compared to patients with no antithrombotic therapy (14.7% and 24.6%, respectively, 33.1% in those with no antithrombotics, p < 0.001). Predicted probabilities of receiving endoscopic treatment, need for transfusion, and number of units transfused did not differ between groups.</p><p><strong>Conclusions: </strong>Patients with anticoagulant therapy more often present with a lower source of Gastrointestinal (GI) bleeding than both those on antiplatelet medications and those with no antithrombotics. However, the presentation of bleeding is similar regardless of any antithrombotic medication or not.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov (NCT05195697), 19/01/2022.</p>\",\"PeriodicalId\":49292,\"journal\":{\"name\":\"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine\",\"volume\":\"33 1\",\"pages\":\"146\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-09-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421751/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13049-025-01431-1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01431-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Presentation of gastrointestinal bleeding in patients with antithrombotic therapy, results from a consecutive retrospective cohort.
Background: Antithrombotic treatment might affect bleeding symptoms, identification of bleeding source and treatment for patients with acute gastrointestinal bleeding. This study aims to investigate possible differences in initial bleeding symptoms, identified bleeding site and treatment of patients with or without antithrombotic medication admitted for gastrointestinal bleeding.
Methods: All consecutive adult patients primarily admitted for gastrointestinal bleeding at Skane University Hospital between 2018-01-01 and 2019-06-31, were included in this study. Data was retrospectively extracted from medical files. Patients were stratified according to antithrombotic therapy (antiplatelet or oral anticoagulants) on admittance or not. Groups were compared using Fisher's exact test, Mann Whitney U-test, Kruskal-Wallis test and logistic regression analysis, including interaction models.
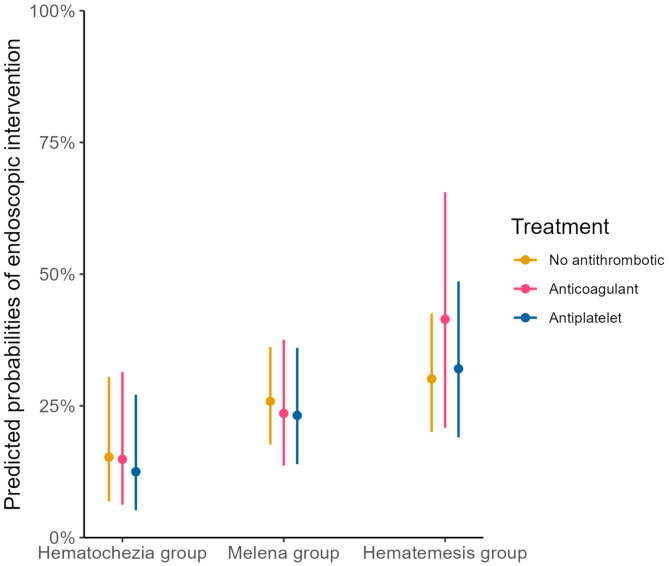
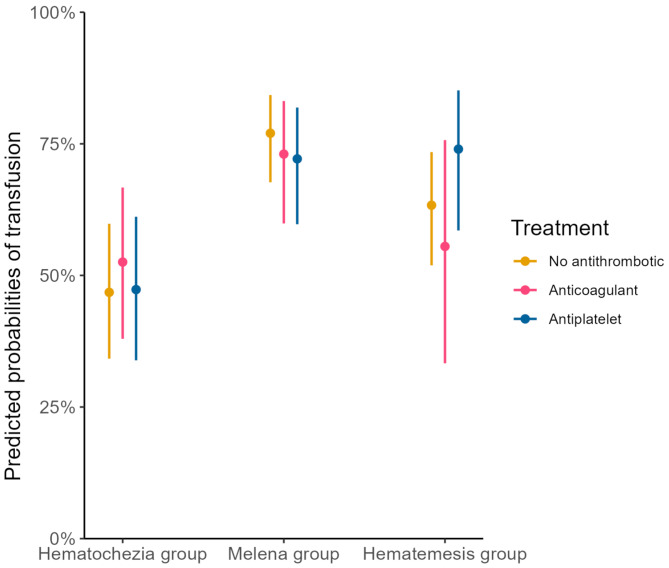
Results: 585 patients were included. Median age was 75 years and a majority (58%) were male. In total, 269 (46%) patients had no antithrombotic medication and 316 (54%) had some kind of antithrombotic medication. Patients with antithrombotic therapy had a higher age and Charlson comorbidity index than those without antithrombotic therapy. However, comparing patients with anticoagulants, antiplatelet medication and no antithrombotics, hemoglobin at arrival (median (interquartile range (IQR)) 99(75-130), 103(85-125) and 100(80-128) respectively, p = 0.851) and Shock index (0.65 (0.50-0.83), 0.67(0.53-0.81) and 0.66 (0.57-0.80) respectively, p = 0.529) did not differ between the groups. Patients with antithrombotic therapy more often presented with hematochezia alone (35.3% and 32.2% for anticoagulant and antiplatelet medications, respectively, 23% for those with no antithrombotics p = 0.017) and less frequently with hematemesis compared to patients with no antithrombotic therapy (14.7% and 24.6%, respectively, 33.1% in those with no antithrombotics, p < 0.001). Predicted probabilities of receiving endoscopic treatment, need for transfusion, and number of units transfused did not differ between groups.
Conclusions: Patients with anticoagulant therapy more often present with a lower source of Gastrointestinal (GI) bleeding than both those on antiplatelet medications and those with no antithrombotics. However, the presentation of bleeding is similar regardless of any antithrombotic medication or not.
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


