Velma Herwanto, Robert Sinto, Leonard Nainggolan, Adityo Susilo, Evy Yunihastuti, Ceva Wicaksono Pitoyo, Hamzah Shatri, Khie Chen Lie
{"title":"免疫反应亚表型预测脓毒症死亡率:一项资源有限的前瞻性研究。","authors":"Velma Herwanto, Robert Sinto, Leonard Nainggolan, Adityo Susilo, Evy Yunihastuti, Ceva Wicaksono Pitoyo, Hamzah Shatri, Khie Chen Lie","doi":"10.1097/CCE.0000000000001315","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Sepsis remains a leading cause of death in infectious cases. The heterogeneity of immune responses is a major challenge in the management and prognostication of patients with sepsis. Identifying distinct immune response subphenotypes using parsimonious classifiers may improve outcome prediction, particularly in resource-limited settings.</p><p><strong>Objectives: </strong>This study aimed to evaluate whether classification of the immune response can serve as a predictor of mortality.</p><p><strong>Design, setting, and participants: </strong>This prospective cohort study was conducted in the emergency department, inpatient wards, and ICU of a tertiary hospital. Adult patients diagnosed with sepsis within the previous 24 hours were included. Exclusion criteria were history of RBC transfusion, major thalassemia, decompensated cirrhosis, hematologic malignancy, or use of immunosuppressive or chronic corticosteroid therapy. Demographic, clinical, and laboratory data-including serum ferritin and monocyte human leukocyte antigen-DR/Human Leukocyte Antigen-DR) (mHLA-DR) levels-were collected.</p><p><strong>Main outcomes and measures: </strong>Subjects were classified into the following immune subphenotypes: macrophage activation-like syndrome (MALS) (if ferritin > 4420 ng/mL), immunoparalysis (if mHLA-DR < 10,000 receptors/cell and ferritin ≤ 4420 ng/mL), and unclassified (if they did not meet the criteria for either MALS or immunoparalysis). The primary outcome was in-hospital mortality.</p><p><strong>Results: </strong>Of the 200 subjects recruited, 54 (27%) were classified into the MALS group, 19 (9.5%) into the immunoparalysis group, and the remainder into the unclassified group. The in-hospital mortality rates for the MALS, immune paralysis, and unclassified groups were 83.3%, 68.4%, and 51.1%, respectively. The proportional hazards assumption was met between the MALS and unclassified groups (crude hazard ratio [HR] 2.3; 95% CI, 1.56-3.35) but not between the immunoparalysis and unclassified groups (crude HR 1.4; 95% CI, 0.76-2.50). After adjusting for confounding variables, MALS's adjusted HR was 1.7 (95% CI, 1.13-2.49; p = 0.01).</p><p><strong>Conclusions and relevance: </strong>The MALS subphenotype is an independent predictor of in-hospital mortality in sepsis.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 9","pages":"e1315"},"PeriodicalIF":2.7000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422772/pdf/","citationCount":"0","resultStr":"{\"title\":\"Immune Response Subphenotyping to Predict Mortality in Sepsis: A Prospective Study in Resource-Limited Setting.\",\"authors\":\"Velma Herwanto, Robert Sinto, Leonard Nainggolan, Adityo Susilo, Evy Yunihastuti, Ceva Wicaksono Pitoyo, Hamzah Shatri, Khie Chen Lie\",\"doi\":\"10.1097/CCE.0000000000001315\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Sepsis remains a leading cause of death in infectious cases. The heterogeneity of immune responses is a major challenge in the management and prognostication of patients with sepsis. Identifying distinct immune response subphenotypes using parsimonious classifiers may improve outcome prediction, particularly in resource-limited settings.</p><p><strong>Objectives: </strong>This study aimed to evaluate whether classification of the immune response can serve as a predictor of mortality.</p><p><strong>Design, setting, and participants: </strong>This prospective cohort study was conducted in the emergency department, inpatient wards, and ICU of a tertiary hospital. Adult patients diagnosed with sepsis within the previous 24 hours were included. Exclusion criteria were history of RBC transfusion, major thalassemia, decompensated cirrhosis, hematologic malignancy, or use of immunosuppressive or chronic corticosteroid therapy. Demographic, clinical, and laboratory data-including serum ferritin and monocyte human leukocyte antigen-DR/Human Leukocyte Antigen-DR) (mHLA-DR) levels-were collected.</p><p><strong>Main outcomes and measures: </strong>Subjects were classified into the following immune subphenotypes: macrophage activation-like syndrome (MALS) (if ferritin > 4420 ng/mL), immunoparalysis (if mHLA-DR < 10,000 receptors/cell and ferritin ≤ 4420 ng/mL), and unclassified (if they did not meet the criteria for either MALS or immunoparalysis). The primary outcome was in-hospital mortality.</p><p><strong>Results: </strong>Of the 200 subjects recruited, 54 (27%) were classified into the MALS group, 19 (9.5%) into the immunoparalysis group, and the remainder into the unclassified group. The in-hospital mortality rates for the MALS, immune paralysis, and unclassified groups were 83.3%, 68.4%, and 51.1%, respectively. The proportional hazards assumption was met between the MALS and unclassified groups (crude hazard ratio [HR] 2.3; 95% CI, 1.56-3.35) but not between the immunoparalysis and unclassified groups (crude HR 1.4; 95% CI, 0.76-2.50). After adjusting for confounding variables, MALS's adjusted HR was 1.7 (95% CI, 1.13-2.49; p = 0.01).</p><p><strong>Conclusions and relevance: </strong>The MALS subphenotype is an independent predictor of in-hospital mortality in sepsis.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 9\",\"pages\":\"e1315\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-09-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422772/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001315\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001315","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Immune Response Subphenotyping to Predict Mortality in Sepsis: A Prospective Study in Resource-Limited Setting.
Importance: Sepsis remains a leading cause of death in infectious cases. The heterogeneity of immune responses is a major challenge in the management and prognostication of patients with sepsis. Identifying distinct immune response subphenotypes using parsimonious classifiers may improve outcome prediction, particularly in resource-limited settings.
Objectives: This study aimed to evaluate whether classification of the immune response can serve as a predictor of mortality.
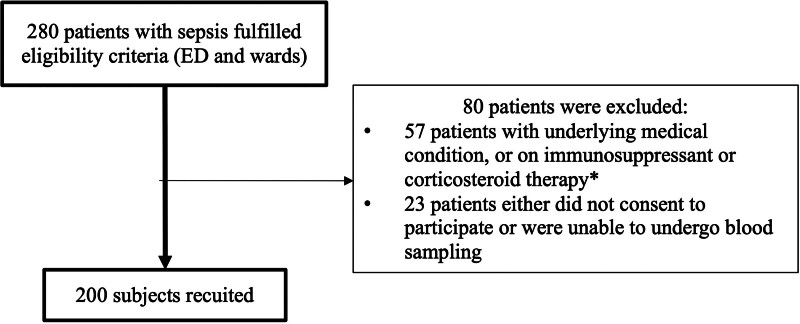
Design, setting, and participants: This prospective cohort study was conducted in the emergency department, inpatient wards, and ICU of a tertiary hospital. Adult patients diagnosed with sepsis within the previous 24 hours were included. Exclusion criteria were history of RBC transfusion, major thalassemia, decompensated cirrhosis, hematologic malignancy, or use of immunosuppressive or chronic corticosteroid therapy. Demographic, clinical, and laboratory data-including serum ferritin and monocyte human leukocyte antigen-DR/Human Leukocyte Antigen-DR) (mHLA-DR) levels-were collected.
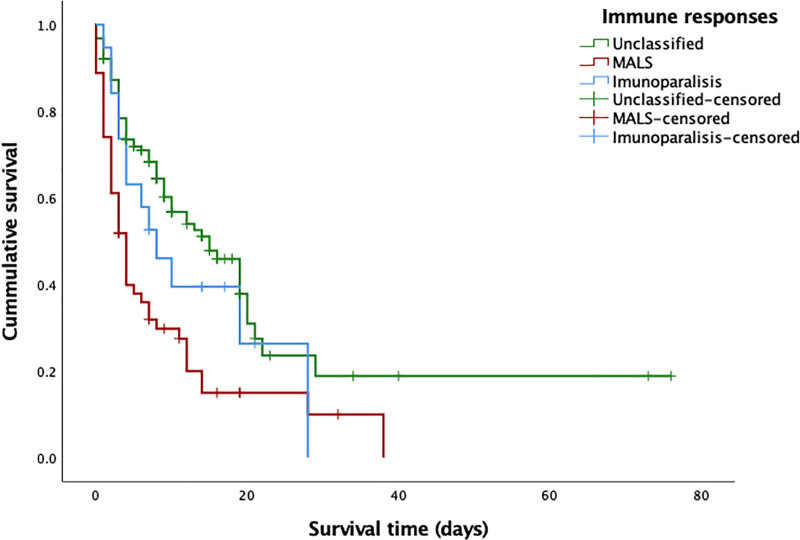
Main outcomes and measures: Subjects were classified into the following immune subphenotypes: macrophage activation-like syndrome (MALS) (if ferritin > 4420 ng/mL), immunoparalysis (if mHLA-DR < 10,000 receptors/cell and ferritin ≤ 4420 ng/mL), and unclassified (if they did not meet the criteria for either MALS or immunoparalysis). The primary outcome was in-hospital mortality.
Results: Of the 200 subjects recruited, 54 (27%) were classified into the MALS group, 19 (9.5%) into the immunoparalysis group, and the remainder into the unclassified group. The in-hospital mortality rates for the MALS, immune paralysis, and unclassified groups were 83.3%, 68.4%, and 51.1%, respectively. The proportional hazards assumption was met between the MALS and unclassified groups (crude hazard ratio [HR] 2.3; 95% CI, 1.56-3.35) but not between the immunoparalysis and unclassified groups (crude HR 1.4; 95% CI, 0.76-2.50). After adjusting for confounding variables, MALS's adjusted HR was 1.7 (95% CI, 1.13-2.49; p = 0.01).
Conclusions and relevance: The MALS subphenotype is an independent predictor of in-hospital mortality in sepsis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


