Archita Ravindranath, Sushil Selvarajan, Sharon Lionel, Anup Joseph Devasia, Anu Korula, Fouzia N Aboobacker, Kavitha M Lakshmi, Poonkuzhali Balasubramanian, Biju George, Vikram Mathews, Aby Abraham, Uday Kulkarni
{"title":"ruxolitinib治疗类固醇难治性急性移植物抗宿主病的实际结果。","authors":"Archita Ravindranath, Sushil Selvarajan, Sharon Lionel, Anup Joseph Devasia, Anu Korula, Fouzia N Aboobacker, Kavitha M Lakshmi, Poonkuzhali Balasubramanian, Biju George, Vikram Mathews, Aby Abraham, Uday Kulkarni","doi":"10.31547/bct-2024-033","DOIUrl":null,"url":null,"abstract":"<p><p>Acute graft-versus-host disease (aGVHD) is a life-threatening complication that can develop after allogeneic hematopoietic stem cell transplantation. Patients with steroid-refractory aGVHD (SR-aGVHD) have an extremely poor prognosis. Ruxolitinib is an approved treatment for SR-aGVHD. However, there is a paucity of real-world data on the clinical outcomes of patients with SR-aGVHD treated with ruxolitinib. We conducted a retrospective analysis using hospital records of the clinical outcomes of patients who underwent stem cell transplantation at our center between January 2021 and December 2022 and developed steroid-refractory aGVHD which was treated with ruxolitinib. During the study period, 381 patients underwent allogeneic stem cell transplantation at our center. Amongst these, 160 (42.0%) developed aGVHD. Of these, 59 (36.8%) had SR-aGVHD and 40 were treated with ruxolitinib. Ruxolitinib therapy was administered after a median of 6 days (range 3-29) from onset of aGVHD. Amongst the 28 patients who survived at day 28 (12 died before the day 28 response could be assessed), a total of 16 patients (57.1%) attained a response (complete response (n=12) or partial response (n=4)). Infectious complications were the most common adverse event (n=39; 97.5%), followed by severe cytopenia (grades 3 to 4) in 25 (62.5%) patients. The median follow-up of the cohort was 5 months (range 1 to 29 months). At the last follow up, 30 (75%) patients died; 3 patients died of progression of steroid-refractory aGVHD, 14 died of progression of aGVHD with infection, 10 died of underlying infection and 3 had disease relapse. From our real-world analysis, we conclude that though the outcomes in patients with SR-aGVHD responding to ruxolitinib are encouraging, there is still a large unmet need for novel strategies for improving outcomes and reducing infection-related mortality, even while there is access to ruxolitinib.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"8 3","pages":"217-224"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414650/pdf/","citationCount":"0","resultStr":"{\"title\":\"REAL-WORLD OUTCOMES OF STEROID-REFRACTORY ACUTE GRAFT-VERSUS-HOST DISEASE TREATED WITH RUXOLITINIB.\",\"authors\":\"Archita Ravindranath, Sushil Selvarajan, Sharon Lionel, Anup Joseph Devasia, Anu Korula, Fouzia N Aboobacker, Kavitha M Lakshmi, Poonkuzhali Balasubramanian, Biju George, Vikram Mathews, Aby Abraham, Uday Kulkarni\",\"doi\":\"10.31547/bct-2024-033\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Acute graft-versus-host disease (aGVHD) is a life-threatening complication that can develop after allogeneic hematopoietic stem cell transplantation. Patients with steroid-refractory aGVHD (SR-aGVHD) have an extremely poor prognosis. Ruxolitinib is an approved treatment for SR-aGVHD. However, there is a paucity of real-world data on the clinical outcomes of patients with SR-aGVHD treated with ruxolitinib. We conducted a retrospective analysis using hospital records of the clinical outcomes of patients who underwent stem cell transplantation at our center between January 2021 and December 2022 and developed steroid-refractory aGVHD which was treated with ruxolitinib. During the study period, 381 patients underwent allogeneic stem cell transplantation at our center. Amongst these, 160 (42.0%) developed aGVHD. Of these, 59 (36.8%) had SR-aGVHD and 40 were treated with ruxolitinib. Ruxolitinib therapy was administered after a median of 6 days (range 3-29) from onset of aGVHD. Amongst the 28 patients who survived at day 28 (12 died before the day 28 response could be assessed), a total of 16 patients (57.1%) attained a response (complete response (n=12) or partial response (n=4)). Infectious complications were the most common adverse event (n=39; 97.5%), followed by severe cytopenia (grades 3 to 4) in 25 (62.5%) patients. The median follow-up of the cohort was 5 months (range 1 to 29 months). At the last follow up, 30 (75%) patients died; 3 patients died of progression of steroid-refractory aGVHD, 14 died of progression of aGVHD with infection, 10 died of underlying infection and 3 had disease relapse. From our real-world analysis, we conclude that though the outcomes in patients with SR-aGVHD responding to ruxolitinib are encouraging, there is still a large unmet need for novel strategies for improving outcomes and reducing infection-related mortality, even while there is access to ruxolitinib.</p>\",\"PeriodicalId\":72423,\"journal\":{\"name\":\"Blood cell therapy\",\"volume\":\"8 3\",\"pages\":\"217-224\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414650/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood cell therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31547/bct-2024-033\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/25 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2024-033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/25 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
REAL-WORLD OUTCOMES OF STEROID-REFRACTORY ACUTE GRAFT-VERSUS-HOST DISEASE TREATED WITH RUXOLITINIB.
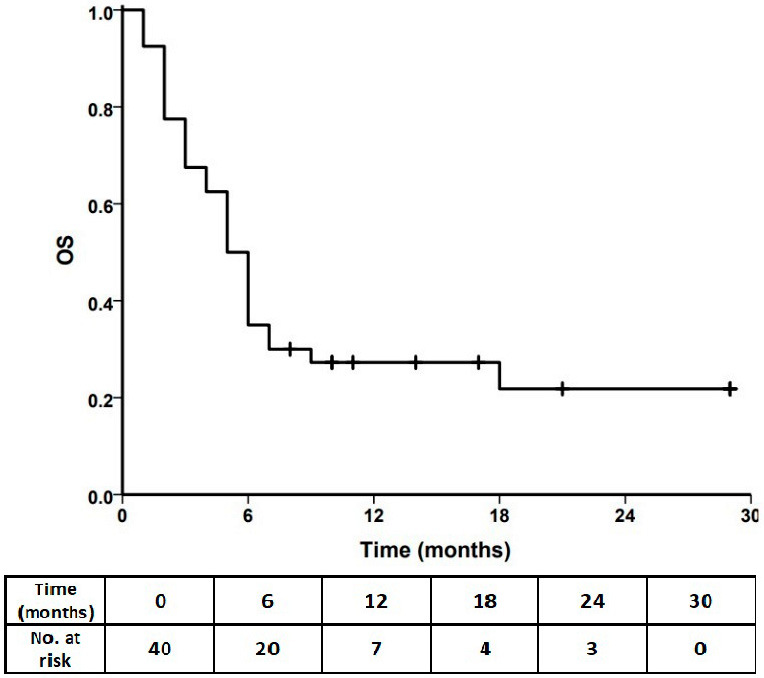
Acute graft-versus-host disease (aGVHD) is a life-threatening complication that can develop after allogeneic hematopoietic stem cell transplantation. Patients with steroid-refractory aGVHD (SR-aGVHD) have an extremely poor prognosis. Ruxolitinib is an approved treatment for SR-aGVHD. However, there is a paucity of real-world data on the clinical outcomes of patients with SR-aGVHD treated with ruxolitinib. We conducted a retrospective analysis using hospital records of the clinical outcomes of patients who underwent stem cell transplantation at our center between January 2021 and December 2022 and developed steroid-refractory aGVHD which was treated with ruxolitinib. During the study period, 381 patients underwent allogeneic stem cell transplantation at our center. Amongst these, 160 (42.0%) developed aGVHD. Of these, 59 (36.8%) had SR-aGVHD and 40 were treated with ruxolitinib. Ruxolitinib therapy was administered after a median of 6 days (range 3-29) from onset of aGVHD. Amongst the 28 patients who survived at day 28 (12 died before the day 28 response could be assessed), a total of 16 patients (57.1%) attained a response (complete response (n=12) or partial response (n=4)). Infectious complications were the most common adverse event (n=39; 97.5%), followed by severe cytopenia (grades 3 to 4) in 25 (62.5%) patients. The median follow-up of the cohort was 5 months (range 1 to 29 months). At the last follow up, 30 (75%) patients died; 3 patients died of progression of steroid-refractory aGVHD, 14 died of progression of aGVHD with infection, 10 died of underlying infection and 3 had disease relapse. From our real-world analysis, we conclude that though the outcomes in patients with SR-aGVHD responding to ruxolitinib are encouraging, there is still a large unmet need for novel strategies for improving outcomes and reducing infection-related mortality, even while there is access to ruxolitinib.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


