Satarupa Mohapatra, Yasser R Abou Mourad, Hannah M Cherniawsky, Shanee S Chung, Donna L Forrest, Gagan Kaila, Florian Kuchenbauer, Katie Lacaria, Joanna MacLean, Stephen H Nantel, Sujaatha Narayanan, Thomas J Nevill, Judith A Rodrigo, Arefeh Rouhi, Claudie Roy, David Sanford, Kevin W Song, Ryan J Stubbins, Cynthia L Toze, Jennifer K White, Deepesh P Lad
{"title":"45岁以上恶性血液病患者清骨髓造血细胞移植结果的种族差异","authors":"Satarupa Mohapatra, Yasser R Abou Mourad, Hannah M Cherniawsky, Shanee S Chung, Donna L Forrest, Gagan Kaila, Florian Kuchenbauer, Katie Lacaria, Joanna MacLean, Stephen H Nantel, Sujaatha Narayanan, Thomas J Nevill, Judith A Rodrigo, Arefeh Rouhi, Claudie Roy, David Sanford, Kevin W Song, Ryan J Stubbins, Cynthia L Toze, Jennifer K White, Deepesh P Lad","doi":"10.31547/bct-2025-001","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The impact of race on outcomes of allogeneic hematopoietic cell transplants (HCT) has long been a field of research. The Center for International Blood and Marrow Transplant Research (CIBMTR) studies have shown worse survival for Black and Hispanic patients within the first year after HCT, but rates evened out for one-year survivors. From our personal experience, we hypothesize that the outcomes of South Asians (age ≥ 45 years) receiving myeloablative conditioning (MAC) are also worse compared to other races.</p><p><strong>Methods: </strong>This is a retrospective single-centre study. All patients (age ≥ 45 years) undergoing MAC-HCT for hematological malignancies from 2011-2022 were included. The primary outcome was overall survival (OS). Secondary outcomes were non-relapse mortality (NRM), incidence of grade 2-4 acute graft versus host disease (GVHD), moderate-severe chronic GVHD and relapse incidence (RI). The survival analysis was performed using Kaplan-Meier analysis and log-rank test. The GVHD, NRM and RI rates were calculated using the cumulative incidence (CI) of competing events and the Gray test. EZR was used for statistical analysis.</p><p><strong>Results: </strong>Of the 483 patients included, there were 28 (5.8%) South Asians (SA), 73 (15.1%), other Asians (East Asians (EA)/Southeast Asians (SEA), and 382 (79.1%) Whites (W). Asians were less likely to get matched unrelated donor-HCT than Whites (SA 21%, EA/SEA 30%, W 45%, <i>p</i>=0.009). The three groups were comparable regarding the recipient and donor sex and performance status. The proportion of SA with HCT-CI ≥ 3 was significantly higher (SA 50%, EA/SEA 37%, W 31%, <i>p</i>=0.03). SA patients were more likely to be obese (body mass index ≥ 30 kg/m<sup>2</sup>) (SA 29%, EA/SEA 5%, W 19%, <i>p</i>=0.005). There were fewer cytomegalovirus (CMV) serological mismatches among the Asians (SA 25%, EA/SEA 26%, W 43%, <i>p</i>=0.009). There was no difference in the conditioning type and CD34 cell dose. However, fewer Asians received Antithymocyte globulin/post-transplant cyclophosphamide as GVHD prophylaxis (SA 39%, EA/SEA 42%, W 45%, <i>p</i>=0.0009). The median OS was significantly shorter in SA (SA 19, EA/SEA 103, W 65 months, <i>p</i>=0.04). The 2-year NRM was significantly higher in SA (SA 35.7%, EA/SEA 13.7%, W 16%, <i>p</i>=0.03). The CI of grade 2-4 acute and moderate-severe chronic GVHD was not significantly different (<i>p</i>=0.7 & 0.6). The 2-year RI was also not significantly different (SA 28.5%, EA/SEA 24.7%, W 28%, <i>p</i>=0.8).</p><p><strong>Conclusion: </strong>Our study confirms that South Asians aged ≥ 45 years have worse survival after MAC-HCT. Supportive care is unable to overcome the differences in the outcomes.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"8 3","pages":"228-233"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414651/pdf/","citationCount":"0","resultStr":"{\"title\":\"Racial Disparity in Myeloablative Hematopoietic Cell Transplantation Outcomes in Patients with Hematological Malignancies Older Than 45 Years.\",\"authors\":\"Satarupa Mohapatra, Yasser R Abou Mourad, Hannah M Cherniawsky, Shanee S Chung, Donna L Forrest, Gagan Kaila, Florian Kuchenbauer, Katie Lacaria, Joanna MacLean, Stephen H Nantel, Sujaatha Narayanan, Thomas J Nevill, Judith A Rodrigo, Arefeh Rouhi, Claudie Roy, David Sanford, Kevin W Song, Ryan J Stubbins, Cynthia L Toze, Jennifer K White, Deepesh P Lad\",\"doi\":\"10.31547/bct-2025-001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The impact of race on outcomes of allogeneic hematopoietic cell transplants (HCT) has long been a field of research. The Center for International Blood and Marrow Transplant Research (CIBMTR) studies have shown worse survival for Black and Hispanic patients within the first year after HCT, but rates evened out for one-year survivors. From our personal experience, we hypothesize that the outcomes of South Asians (age ≥ 45 years) receiving myeloablative conditioning (MAC) are also worse compared to other races.</p><p><strong>Methods: </strong>This is a retrospective single-centre study. All patients (age ≥ 45 years) undergoing MAC-HCT for hematological malignancies from 2011-2022 were included. The primary outcome was overall survival (OS). Secondary outcomes were non-relapse mortality (NRM), incidence of grade 2-4 acute graft versus host disease (GVHD), moderate-severe chronic GVHD and relapse incidence (RI). The survival analysis was performed using Kaplan-Meier analysis and log-rank test. The GVHD, NRM and RI rates were calculated using the cumulative incidence (CI) of competing events and the Gray test. EZR was used for statistical analysis.</p><p><strong>Results: </strong>Of the 483 patients included, there were 28 (5.8%) South Asians (SA), 73 (15.1%), other Asians (East Asians (EA)/Southeast Asians (SEA), and 382 (79.1%) Whites (W). Asians were less likely to get matched unrelated donor-HCT than Whites (SA 21%, EA/SEA 30%, W 45%, <i>p</i>=0.009). The three groups were comparable regarding the recipient and donor sex and performance status. The proportion of SA with HCT-CI ≥ 3 was significantly higher (SA 50%, EA/SEA 37%, W 31%, <i>p</i>=0.03). SA patients were more likely to be obese (body mass index ≥ 30 kg/m<sup>2</sup>) (SA 29%, EA/SEA 5%, W 19%, <i>p</i>=0.005). There were fewer cytomegalovirus (CMV) serological mismatches among the Asians (SA 25%, EA/SEA 26%, W 43%, <i>p</i>=0.009). There was no difference in the conditioning type and CD34 cell dose. However, fewer Asians received Antithymocyte globulin/post-transplant cyclophosphamide as GVHD prophylaxis (SA 39%, EA/SEA 42%, W 45%, <i>p</i>=0.0009). The median OS was significantly shorter in SA (SA 19, EA/SEA 103, W 65 months, <i>p</i>=0.04). The 2-year NRM was significantly higher in SA (SA 35.7%, EA/SEA 13.7%, W 16%, <i>p</i>=0.03). The CI of grade 2-4 acute and moderate-severe chronic GVHD was not significantly different (<i>p</i>=0.7 & 0.6). The 2-year RI was also not significantly different (SA 28.5%, EA/SEA 24.7%, W 28%, <i>p</i>=0.8).</p><p><strong>Conclusion: </strong>Our study confirms that South Asians aged ≥ 45 years have worse survival after MAC-HCT. Supportive care is unable to overcome the differences in the outcomes.</p>\",\"PeriodicalId\":72423,\"journal\":{\"name\":\"Blood cell therapy\",\"volume\":\"8 3\",\"pages\":\"228-233\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414651/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood cell therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31547/bct-2025-001\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/25 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2025-001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/25 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
种族对同种异体造血细胞移植(HCT)结果的影响一直是一个研究领域。国际血液和骨髓移植研究中心(CIBMTR)的研究表明,黑人和西班牙裔患者在HCT后的第一年生存率较低,但一年内生存率持平。根据我们的个人经验,我们假设南亚人(年龄≥45岁)接受骨髓清除条件反射(MAC)的结果也比其他种族更差。方法:这是一项回顾性单中心研究。2011-2022年期间接受MAC-HCT检查的所有恶性血液病患者(年龄≥45岁)均被纳入研究。主要终点是总生存期(OS)。次要结局为非复发死亡率(NRM)、2-4级急性移植物抗宿主病(GVHD)、中重度慢性移植物抗宿主病(GVHD)和复发率(RI)。生存率分析采用Kaplan-Meier分析和log-rank检验。GVHD、NRM和RI的计算采用竞争事件的累积发生率(CI)和Gray检验。采用EZR进行统计分析。结果:纳入的483例患者中,南亚人(SA) 28例(5.8%),其他亚洲人(东亚人(EA)/东南亚人(SEA)) 73例(15.1%),白人(W) 382例(79.1%)。亚洲人获得匹配的非亲属供者- hct的可能性低于白人(SA 21%, EA/SEA 30%, W 45%, p=0.009)。三组在受者和供者的性别和表现状况方面具有可比性。HCT-CI≥3的SA比例显著高于对照组(SA 50%, EA/SEA 37%, W 31%, p=0.03)。SA患者更易发生肥胖(体重指数≥30 kg/m2) (SA 29%, EA/SEA 5%, W 19%, p=0.005)。亚洲人巨细胞病毒(CMV)血清学不匹配较少(SA 25%, EA/SEA 26%, W 43%, p=0.009)。调理类型和CD34细胞剂量均无差异。然而,较少的亚洲人接受抗胸腺细胞球蛋白/移植后环磷酰胺作为GVHD预防(SA 39%, EA/SEA 42%, W 45%, p=0.0009)。SA组的中位生存期显著缩短(SA 19个月,EA/SEA 103个月,W 65个月,p=0.04)。SA组2年NRM显著高于SA组(SA 35.7%, EA/SEA 13.7%, W 16%, p=0.03)。2-4级急性和中重度慢性GVHD的CI差异无统计学意义(p=0.7 & 0.6)。2年RI也无显著差异(SA 28.5%, EA/SEA 24.7%, W 28%, p=0.8)。结论:我们的研究证实,年龄≥45岁的南亚人在MAC-HCT后生存率较差。支持性护理无法克服结果上的差异。
Racial Disparity in Myeloablative Hematopoietic Cell Transplantation Outcomes in Patients with Hematological Malignancies Older Than 45 Years.
Introduction: The impact of race on outcomes of allogeneic hematopoietic cell transplants (HCT) has long been a field of research. The Center for International Blood and Marrow Transplant Research (CIBMTR) studies have shown worse survival for Black and Hispanic patients within the first year after HCT, but rates evened out for one-year survivors. From our personal experience, we hypothesize that the outcomes of South Asians (age ≥ 45 years) receiving myeloablative conditioning (MAC) are also worse compared to other races.
Methods: This is a retrospective single-centre study. All patients (age ≥ 45 years) undergoing MAC-HCT for hematological malignancies from 2011-2022 were included. The primary outcome was overall survival (OS). Secondary outcomes were non-relapse mortality (NRM), incidence of grade 2-4 acute graft versus host disease (GVHD), moderate-severe chronic GVHD and relapse incidence (RI). The survival analysis was performed using Kaplan-Meier analysis and log-rank test. The GVHD, NRM and RI rates were calculated using the cumulative incidence (CI) of competing events and the Gray test. EZR was used for statistical analysis.
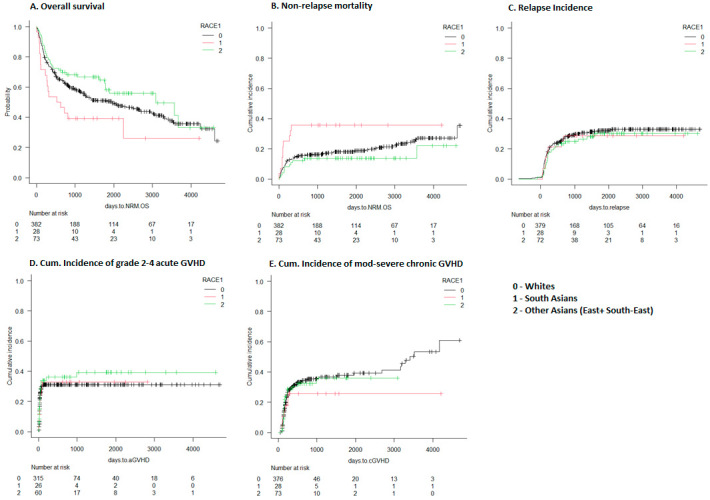
Results: Of the 483 patients included, there were 28 (5.8%) South Asians (SA), 73 (15.1%), other Asians (East Asians (EA)/Southeast Asians (SEA), and 382 (79.1%) Whites (W). Asians were less likely to get matched unrelated donor-HCT than Whites (SA 21%, EA/SEA 30%, W 45%, p=0.009). The three groups were comparable regarding the recipient and donor sex and performance status. The proportion of SA with HCT-CI ≥ 3 was significantly higher (SA 50%, EA/SEA 37%, W 31%, p=0.03). SA patients were more likely to be obese (body mass index ≥ 30 kg/m2) (SA 29%, EA/SEA 5%, W 19%, p=0.005). There were fewer cytomegalovirus (CMV) serological mismatches among the Asians (SA 25%, EA/SEA 26%, W 43%, p=0.009). There was no difference in the conditioning type and CD34 cell dose. However, fewer Asians received Antithymocyte globulin/post-transplant cyclophosphamide as GVHD prophylaxis (SA 39%, EA/SEA 42%, W 45%, p=0.0009). The median OS was significantly shorter in SA (SA 19, EA/SEA 103, W 65 months, p=0.04). The 2-year NRM was significantly higher in SA (SA 35.7%, EA/SEA 13.7%, W 16%, p=0.03). The CI of grade 2-4 acute and moderate-severe chronic GVHD was not significantly different (p=0.7 & 0.6). The 2-year RI was also not significantly different (SA 28.5%, EA/SEA 24.7%, W 28%, p=0.8).
Conclusion: Our study confirms that South Asians aged ≥ 45 years have worse survival after MAC-HCT. Supportive care is unable to overcome the differences in the outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


