Mark P Cote, Kaitlyn E Holly, Roman J Schoenfeld, Matthew R Bryan, Malina O Hatton, Mitchel B Harris, Tracey P Koehlmoos, Andrew J Schoenfeld
{"title":"建模肌肉骨骼战斗伤亡护理:北约创伤系统性能在大规模作战行动。","authors":"Mark P Cote, Kaitlyn E Holly, Roman J Schoenfeld, Matthew R Bryan, Malina O Hatton, Mitchel B Harris, Tracey P Koehlmoos, Andrew J Schoenfeld","doi":"10.2106/JBJS.OA.25.00194","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>It is unclear whether the current North Atlantic Treaty Organization (NATO) trauma system will be effective in the setting of Large-Scale Combat Operations (LSCO). We sought to model the efficacy of the NATO trauma system in the setting of LSCO. We also intended to model novel scenarios that could better adapt the current system to LSCO.</p><p><strong>Methods: </strong>We developed a discrete-event simulation model for patients with combat musculoskeletal injuries treated within the standard NATO system. The primary outcome of the model was survival. The model's health states were characterized as stable, hypovolemia, sepsis, shock, or death. The model simulated combat intensity by increasing the number of casualties up to 192 casualties per 24 hours. We explored how an augmented system (FC) and Field Hospital (FH) moved closer to the battlefront would change performance.</p><p><strong>Results: </strong>Mortality rates rose precipitously from a 10% baseline to 61% at 12 casualties per 24 hours in the base model. This performance was not significantly different from that of the FC model at any casualty rate. Successful evacuation of casualties was significantly more for the FH model versus the base model at 12 casualties/24 hours (47.5% vs. 39%; p = 0.046), 48 casualties/24 hours (45.5% vs. 33%; p = 0.008), and 192 casualties/24 hours (25% vs. 15.5%; p = 0.02).</p><p><strong>Conclusions: </strong>The current NATO model experiences high rates of mortality in LSCO. The most effective modification entails situating Field Hospitals within one-hour of ground transport from the battlefront.</p><p><strong>Level of evidence: </strong>Level III. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 3","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417006/pdf/","citationCount":"0","resultStr":"{\"title\":\"Modeling Musculoskeletal Combat Casualty Care: NATO Trauma System Performance in Large Scale Combat Operations.\",\"authors\":\"Mark P Cote, Kaitlyn E Holly, Roman J Schoenfeld, Matthew R Bryan, Malina O Hatton, Mitchel B Harris, Tracey P Koehlmoos, Andrew J Schoenfeld\",\"doi\":\"10.2106/JBJS.OA.25.00194\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>It is unclear whether the current North Atlantic Treaty Organization (NATO) trauma system will be effective in the setting of Large-Scale Combat Operations (LSCO). We sought to model the efficacy of the NATO trauma system in the setting of LSCO. We also intended to model novel scenarios that could better adapt the current system to LSCO.</p><p><strong>Methods: </strong>We developed a discrete-event simulation model for patients with combat musculoskeletal injuries treated within the standard NATO system. The primary outcome of the model was survival. The model's health states were characterized as stable, hypovolemia, sepsis, shock, or death. The model simulated combat intensity by increasing the number of casualties up to 192 casualties per 24 hours. We explored how an augmented system (FC) and Field Hospital (FH) moved closer to the battlefront would change performance.</p><p><strong>Results: </strong>Mortality rates rose precipitously from a 10% baseline to 61% at 12 casualties per 24 hours in the base model. This performance was not significantly different from that of the FC model at any casualty rate. Successful evacuation of casualties was significantly more for the FH model versus the base model at 12 casualties/24 hours (47.5% vs. 39%; p = 0.046), 48 casualties/24 hours (45.5% vs. 33%; p = 0.008), and 192 casualties/24 hours (25% vs. 15.5%; p = 0.02).</p><p><strong>Conclusions: </strong>The current NATO model experiences high rates of mortality in LSCO. The most effective modification entails situating Field Hospitals within one-hour of ground transport from the battlefront.</p><p><strong>Level of evidence: </strong>Level III. See Instructions for Authors for a complete description of levels of evidence.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"10 3\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-09-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417006/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.25.00194\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.25.00194","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:目前尚不清楚北大西洋公约组织(NATO)的创伤系统在大规模作战行动(LSCO)中是否有效。我们试图模拟北约创伤系统在LSCO环境下的疗效。我们还打算建立新的场景模型,使当前系统更好地适应LSCO。方法:我们开发了一个离散事件模拟模型,用于在标准北约系统内治疗的战斗肌肉骨骼损伤患者。该模型的主要结局是生存。模型的健康状态为稳定、低血容量、败血症、休克或死亡。该模型将每24小时的伤亡人数增加到192人,模拟了战斗强度。我们探讨了增强系统(FC)和野战医院(FH)向前线移动将如何改变性能。结果:在基础模型中,每24小时有12人死亡,死亡率从10%的基线急剧上升到61%。在任何伤亡率下,这一性能与FC模型没有显著差异。与基础模型相比,FH模型在12人/24小时(47.5% vs. 39%, p = 0.046)、48人/24小时(45.5% vs. 33%, p = 0.008)和192人/24小时(25% vs. 15.5%, p = 0.02)的成功疏散伤亡人数明显更多。结论:目前的北约模型在LSCO中经历了高死亡率。最有效的修改是将野战医院设在离前线地面交通不到一小时的地方。证据等级:三级。有关证据水平的完整描述,请参见作者说明。
Modeling Musculoskeletal Combat Casualty Care: NATO Trauma System Performance in Large Scale Combat Operations.
Background: It is unclear whether the current North Atlantic Treaty Organization (NATO) trauma system will be effective in the setting of Large-Scale Combat Operations (LSCO). We sought to model the efficacy of the NATO trauma system in the setting of LSCO. We also intended to model novel scenarios that could better adapt the current system to LSCO.
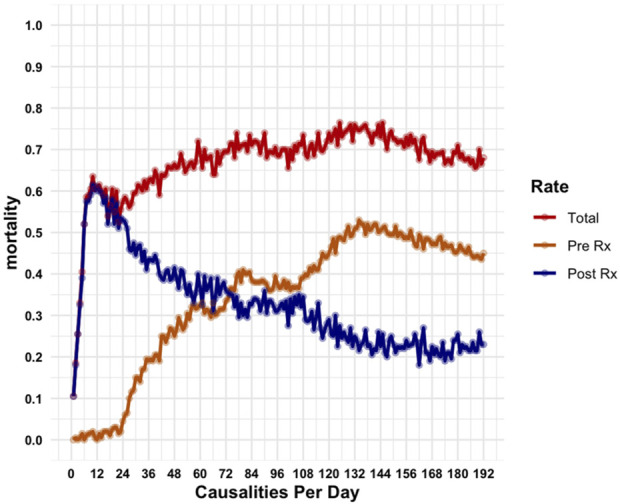
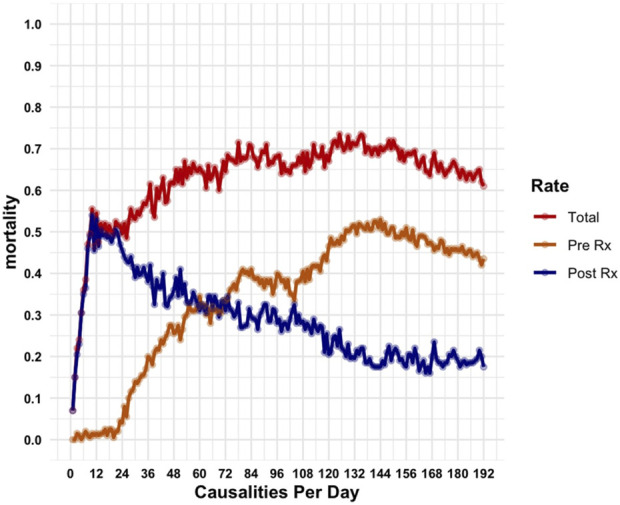
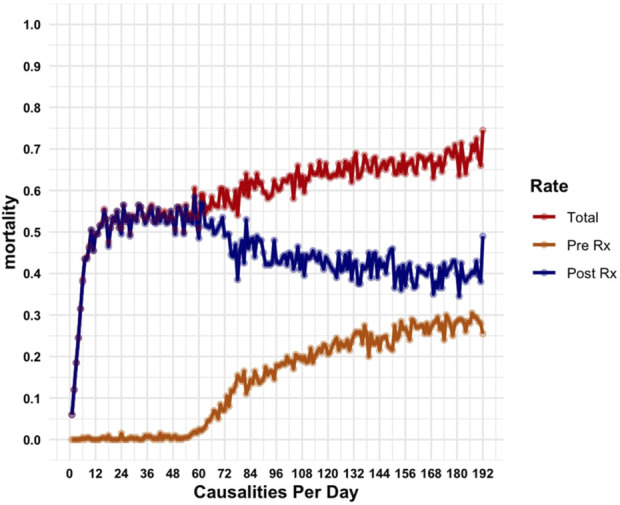
Methods: We developed a discrete-event simulation model for patients with combat musculoskeletal injuries treated within the standard NATO system. The primary outcome of the model was survival. The model's health states were characterized as stable, hypovolemia, sepsis, shock, or death. The model simulated combat intensity by increasing the number of casualties up to 192 casualties per 24 hours. We explored how an augmented system (FC) and Field Hospital (FH) moved closer to the battlefront would change performance.
Results: Mortality rates rose precipitously from a 10% baseline to 61% at 12 casualties per 24 hours in the base model. This performance was not significantly different from that of the FC model at any casualty rate. Successful evacuation of casualties was significantly more for the FH model versus the base model at 12 casualties/24 hours (47.5% vs. 39%; p = 0.046), 48 casualties/24 hours (45.5% vs. 33%; p = 0.008), and 192 casualties/24 hours (25% vs. 15.5%; p = 0.02).
Conclusions: The current NATO model experiences high rates of mortality in LSCO. The most effective modification entails situating Field Hospitals within one-hour of ground transport from the battlefront.
Level of evidence: Level III. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


