{"title":"在脑癌治疗中什么时候需要肾活检?","authors":"Catarina Oliveira-Silva, Johanna Viana, Claudia Coelho, Roberto Silva, Luís Falcão, Joana Rocha, Bárbara Ribeiro","doi":"10.12890/2025_005565","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Bevacizumab is a monoclonal antibody that targets vascular endothelial growth factor (VEGF) and is widely used in oncology for its anti-angiogenic properties. However, VEGF inhibition may result in significant nephrotoxicity, including thrombotic microangiopathy (TMA). While systemic TMA is well-described, isolated renal-limited TMA remains under recognised.</p><p><strong>Case description: </strong>We present a 46-year-old woman with WHO grade IV IDH-wildtype EGFR-amplified gliosarcoma. She received second-line treatment with bevacizumab and, after 12 months of therapy, developed progressive hypertension and nephrotic-range proteinuria up to 6.2 g/day, with normal renal function and without anaemia or thrombocytopenia. A kidney biopsy revealed glomerular microangiopathy, and a diagnosis of bevacizumab-associated renal-limited TMA was established. Given the stability of the intracranial disease, the drug was discontinued with complete resolution of proteinuria after seven months.</p><p><strong>Conclusion: </strong>Anti-VEGF therapy causes renal TMA and may present with nephrotic-range proteinuria associated with a pattern of glomerular microangiopathy. Recognising anti-VEGF-associated nephrotoxicity is essential in the differential diagnosis of proteinuria in cancer patients, and kidney biopsy is fundamental for guiding clinical decisions. Drug cessation led to the complete resolution of proteinuria.</p><p><strong>Learning points: </strong>Bevacizumab can cause renal-limited thrombotic microangiopathy and may present with nephrotic-range proteinuria, without renal dysfunction.Kidney biopsy is essential to distinguish drug-induced thrombotic microangiopathy from malignancy-associated nephropathies in cancer patients.Early recognition and drug discontinuation can lead to complete proteinuria resolution.</p>","PeriodicalId":11908,"journal":{"name":"European journal of case reports in internal medicine","volume":"12 9","pages":"005565"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416784/pdf/","citationCount":"0","resultStr":"{\"title\":\"When is A Kidney Biopsy Indicated During the Treatment of Brain Cancer?\",\"authors\":\"Catarina Oliveira-Silva, Johanna Viana, Claudia Coelho, Roberto Silva, Luís Falcão, Joana Rocha, Bárbara Ribeiro\",\"doi\":\"10.12890/2025_005565\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Bevacizumab is a monoclonal antibody that targets vascular endothelial growth factor (VEGF) and is widely used in oncology for its anti-angiogenic properties. However, VEGF inhibition may result in significant nephrotoxicity, including thrombotic microangiopathy (TMA). While systemic TMA is well-described, isolated renal-limited TMA remains under recognised.</p><p><strong>Case description: </strong>We present a 46-year-old woman with WHO grade IV IDH-wildtype EGFR-amplified gliosarcoma. She received second-line treatment with bevacizumab and, after 12 months of therapy, developed progressive hypertension and nephrotic-range proteinuria up to 6.2 g/day, with normal renal function and without anaemia or thrombocytopenia. A kidney biopsy revealed glomerular microangiopathy, and a diagnosis of bevacizumab-associated renal-limited TMA was established. Given the stability of the intracranial disease, the drug was discontinued with complete resolution of proteinuria after seven months.</p><p><strong>Conclusion: </strong>Anti-VEGF therapy causes renal TMA and may present with nephrotic-range proteinuria associated with a pattern of glomerular microangiopathy. Recognising anti-VEGF-associated nephrotoxicity is essential in the differential diagnosis of proteinuria in cancer patients, and kidney biopsy is fundamental for guiding clinical decisions. Drug cessation led to the complete resolution of proteinuria.</p><p><strong>Learning points: </strong>Bevacizumab can cause renal-limited thrombotic microangiopathy and may present with nephrotic-range proteinuria, without renal dysfunction.Kidney biopsy is essential to distinguish drug-induced thrombotic microangiopathy from malignancy-associated nephropathies in cancer patients.Early recognition and drug discontinuation can lead to complete proteinuria resolution.</p>\",\"PeriodicalId\":11908,\"journal\":{\"name\":\"European journal of case reports in internal medicine\",\"volume\":\"12 9\",\"pages\":\"005565\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416784/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of case reports in internal medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12890/2025_005565\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of case reports in internal medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12890/2025_005565","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
When is A Kidney Biopsy Indicated During the Treatment of Brain Cancer?
Introduction: Bevacizumab is a monoclonal antibody that targets vascular endothelial growth factor (VEGF) and is widely used in oncology for its anti-angiogenic properties. However, VEGF inhibition may result in significant nephrotoxicity, including thrombotic microangiopathy (TMA). While systemic TMA is well-described, isolated renal-limited TMA remains under recognised.
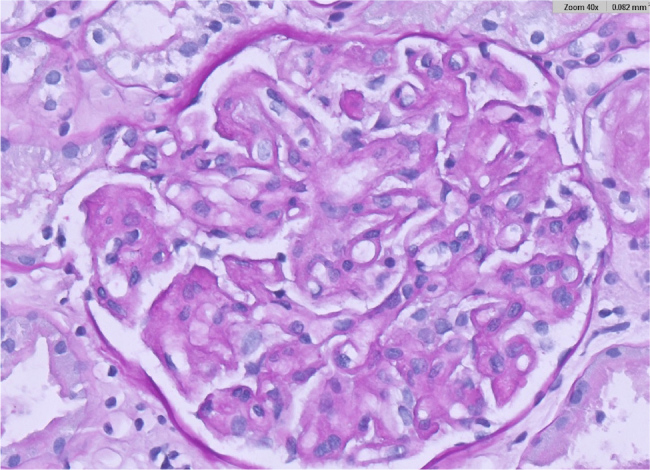
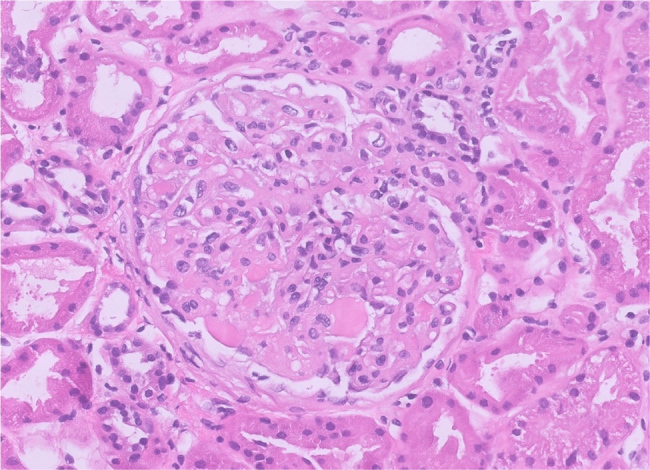
Case description: We present a 46-year-old woman with WHO grade IV IDH-wildtype EGFR-amplified gliosarcoma. She received second-line treatment with bevacizumab and, after 12 months of therapy, developed progressive hypertension and nephrotic-range proteinuria up to 6.2 g/day, with normal renal function and without anaemia or thrombocytopenia. A kidney biopsy revealed glomerular microangiopathy, and a diagnosis of bevacizumab-associated renal-limited TMA was established. Given the stability of the intracranial disease, the drug was discontinued with complete resolution of proteinuria after seven months.
Conclusion: Anti-VEGF therapy causes renal TMA and may present with nephrotic-range proteinuria associated with a pattern of glomerular microangiopathy. Recognising anti-VEGF-associated nephrotoxicity is essential in the differential diagnosis of proteinuria in cancer patients, and kidney biopsy is fundamental for guiding clinical decisions. Drug cessation led to the complete resolution of proteinuria.
Learning points: Bevacizumab can cause renal-limited thrombotic microangiopathy and may present with nephrotic-range proteinuria, without renal dysfunction.Kidney biopsy is essential to distinguish drug-induced thrombotic microangiopathy from malignancy-associated nephropathies in cancer patients.Early recognition and drug discontinuation can lead to complete proteinuria resolution.
期刊介绍:
The European Journal of Case Reports in Internal Medicine is an official journal of the European Federation of Internal Medicine (EFIM), representing 35 national societies from 33 European countries. The Journal''s mission is to promote the best medical practice and innovation in the field of acute and general medicine. It also provides a forum for internal medicine doctors where they can share new approaches with the aim of improving diagnostic and clinical skills in this field. EJCRIM welcomes high-quality case reports describing unusual or complex cases that an internist may encounter in everyday practice. The cases should either demonstrate the appropriateness of a diagnostic/therapeutic approach, describe a new procedure or maneuver, or show unusual manifestations of a disease or unexpected reactions. The Journal only accepts and publishes those case reports whose learning points provide new insight and/or contribute to advancing medical knowledge both in terms of diagnostics and therapeutic approaches. Case reports of medical errors, therefore, are also welcome as long as they provide innovative measures on how to prevent them in the current practice (Instructive Errors). The Journal may also consider brief and reasoned reports on issues relevant to the practice of Internal Medicine, as well as Abstracts submitted to the scientific meetings of acknowledged medical societies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


