Mirko Lischer, Marten Trendelenburg, Özgür Yaldizli, Nikolaos S Avramiotis, Grischa Marti, Anna Vital
{"title":"1例副肿瘤脑炎患者1型单纯疱疹病毒的误检。","authors":"Mirko Lischer, Marten Trendelenburg, Özgür Yaldizli, Nikolaos S Avramiotis, Grischa Marti, Anna Vital","doi":"10.12890/2025_005705","DOIUrl":null,"url":null,"abstract":"<p><p>Encephalitis is a potentially life-threatening condition with infectious or autoimmune aetiologies. Autoimmune encephalitis includes paraneoplastic variants associated with specific onconeural antibodies such as anti-Hu, frequently linked to malignancies. Herpes simplex virus type 1 (HSV-1) is the leading infectious cause in adults. Differentiating between these aetiologies can be challenging. We report the case of an 88-year-old woman admitted with confusion following a fall. Initial evaluation showed clinical signs consistent with encephalitis. During hospitalisation, a seizure was witnessed. Cerebrospinal fluid (CSF) analysis revealed mild pleocytosis, but no infectious agent was detected, and brain imaging revealed no significant abnormalities. After initial improvement under antiepileptic therapy, the patient experienced worsening cognitive dysfunction. Repeat CSF testing 4 weeks after initial symptom onset showed even milder pleocytosis but was positive for HSV-1 and magnetic resonance imaging showed bilateral hippocampal hyperintensities. Analysis of the first CSF sample retrospectively revealed high-titer anti-Hu antibodies. Positron emission tomography-computed tomography scan identified a hypermetabolic lung lesion and para-aortic lymph node, with biopsy confirming the diagnosis of small cell lung cancer. Immunosuppressive and oncologic treatment led to transient improvement, followed by progressive neurological deterioration. Supportive care was ultimately prioritized. This case underscores the diagnostic challenges of encephalitis, especially when autoimmune and infectious features overlap, and diagnostic findings are misleading. Detection of HSV-1 should not delay the investigation of alternative causes of encephalitis in the absence of typical HSV-related features. Early recognition of paraneoplastic encephalitis is critical, as neurologic symptoms may precede the diagnosis of underlying malignancy.</p><p><strong>Learning points: </strong>Onconeural antibodies, such as anti-Hu antibodies, are an under-recognized cause of encephalitis and should be specifically tested for when an autoimmune encephalitis is clinically suspected.Detection of anti-Hu antibodies mandates a comprehensive malignancy workup.A positive herpes simplex virus type 1 polymerase chain reaction in cerebrospinal fluid does not definitively confirm active infection and must always be interpreted in conjunction with the patient's clinical presentation.</p>","PeriodicalId":11908,"journal":{"name":"European journal of case reports in internal medicine","volume":"12 9","pages":"005705"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416775/pdf/","citationCount":"0","resultStr":"{\"title\":\"Misleading Detection of Herpes Simplex Virus Type 1 In A Patient with Paraneoplastic Encephalitis.\",\"authors\":\"Mirko Lischer, Marten Trendelenburg, Özgür Yaldizli, Nikolaos S Avramiotis, Grischa Marti, Anna Vital\",\"doi\":\"10.12890/2025_005705\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Encephalitis is a potentially life-threatening condition with infectious or autoimmune aetiologies. Autoimmune encephalitis includes paraneoplastic variants associated with specific onconeural antibodies such as anti-Hu, frequently linked to malignancies. Herpes simplex virus type 1 (HSV-1) is the leading infectious cause in adults. Differentiating between these aetiologies can be challenging. We report the case of an 88-year-old woman admitted with confusion following a fall. Initial evaluation showed clinical signs consistent with encephalitis. During hospitalisation, a seizure was witnessed. Cerebrospinal fluid (CSF) analysis revealed mild pleocytosis, but no infectious agent was detected, and brain imaging revealed no significant abnormalities. After initial improvement under antiepileptic therapy, the patient experienced worsening cognitive dysfunction. Repeat CSF testing 4 weeks after initial symptom onset showed even milder pleocytosis but was positive for HSV-1 and magnetic resonance imaging showed bilateral hippocampal hyperintensities. Analysis of the first CSF sample retrospectively revealed high-titer anti-Hu antibodies. Positron emission tomography-computed tomography scan identified a hypermetabolic lung lesion and para-aortic lymph node, with biopsy confirming the diagnosis of small cell lung cancer. Immunosuppressive and oncologic treatment led to transient improvement, followed by progressive neurological deterioration. Supportive care was ultimately prioritized. This case underscores the diagnostic challenges of encephalitis, especially when autoimmune and infectious features overlap, and diagnostic findings are misleading. Detection of HSV-1 should not delay the investigation of alternative causes of encephalitis in the absence of typical HSV-related features. Early recognition of paraneoplastic encephalitis is critical, as neurologic symptoms may precede the diagnosis of underlying malignancy.</p><p><strong>Learning points: </strong>Onconeural antibodies, such as anti-Hu antibodies, are an under-recognized cause of encephalitis and should be specifically tested for when an autoimmune encephalitis is clinically suspected.Detection of anti-Hu antibodies mandates a comprehensive malignancy workup.A positive herpes simplex virus type 1 polymerase chain reaction in cerebrospinal fluid does not definitively confirm active infection and must always be interpreted in conjunction with the patient's clinical presentation.</p>\",\"PeriodicalId\":11908,\"journal\":{\"name\":\"European journal of case reports in internal medicine\",\"volume\":\"12 9\",\"pages\":\"005705\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416775/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of case reports in internal medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12890/2025_005705\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of case reports in internal medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12890/2025_005705","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Misleading Detection of Herpes Simplex Virus Type 1 In A Patient with Paraneoplastic Encephalitis.
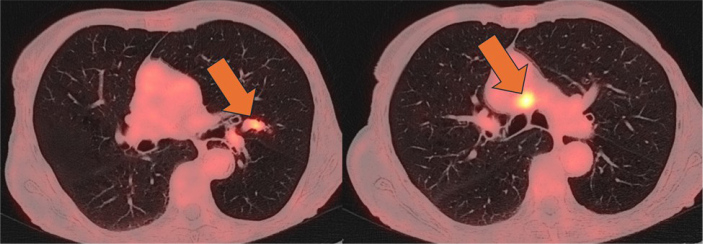
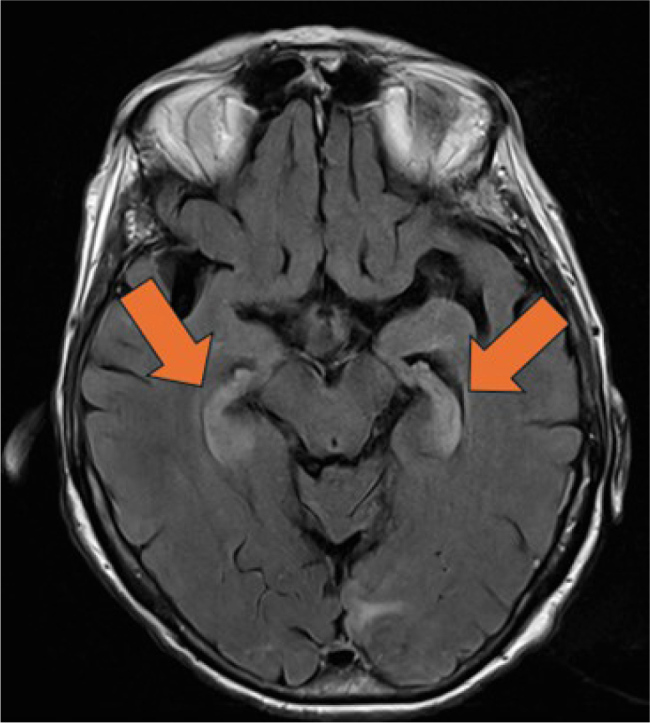
Encephalitis is a potentially life-threatening condition with infectious or autoimmune aetiologies. Autoimmune encephalitis includes paraneoplastic variants associated with specific onconeural antibodies such as anti-Hu, frequently linked to malignancies. Herpes simplex virus type 1 (HSV-1) is the leading infectious cause in adults. Differentiating between these aetiologies can be challenging. We report the case of an 88-year-old woman admitted with confusion following a fall. Initial evaluation showed clinical signs consistent with encephalitis. During hospitalisation, a seizure was witnessed. Cerebrospinal fluid (CSF) analysis revealed mild pleocytosis, but no infectious agent was detected, and brain imaging revealed no significant abnormalities. After initial improvement under antiepileptic therapy, the patient experienced worsening cognitive dysfunction. Repeat CSF testing 4 weeks after initial symptom onset showed even milder pleocytosis but was positive for HSV-1 and magnetic resonance imaging showed bilateral hippocampal hyperintensities. Analysis of the first CSF sample retrospectively revealed high-titer anti-Hu antibodies. Positron emission tomography-computed tomography scan identified a hypermetabolic lung lesion and para-aortic lymph node, with biopsy confirming the diagnosis of small cell lung cancer. Immunosuppressive and oncologic treatment led to transient improvement, followed by progressive neurological deterioration. Supportive care was ultimately prioritized. This case underscores the diagnostic challenges of encephalitis, especially when autoimmune and infectious features overlap, and diagnostic findings are misleading. Detection of HSV-1 should not delay the investigation of alternative causes of encephalitis in the absence of typical HSV-related features. Early recognition of paraneoplastic encephalitis is critical, as neurologic symptoms may precede the diagnosis of underlying malignancy.
Learning points: Onconeural antibodies, such as anti-Hu antibodies, are an under-recognized cause of encephalitis and should be specifically tested for when an autoimmune encephalitis is clinically suspected.Detection of anti-Hu antibodies mandates a comprehensive malignancy workup.A positive herpes simplex virus type 1 polymerase chain reaction in cerebrospinal fluid does not definitively confirm active infection and must always be interpreted in conjunction with the patient's clinical presentation.
期刊介绍:
The European Journal of Case Reports in Internal Medicine is an official journal of the European Federation of Internal Medicine (EFIM), representing 35 national societies from 33 European countries. The Journal''s mission is to promote the best medical practice and innovation in the field of acute and general medicine. It also provides a forum for internal medicine doctors where they can share new approaches with the aim of improving diagnostic and clinical skills in this field. EJCRIM welcomes high-quality case reports describing unusual or complex cases that an internist may encounter in everyday practice. The cases should either demonstrate the appropriateness of a diagnostic/therapeutic approach, describe a new procedure or maneuver, or show unusual manifestations of a disease or unexpected reactions. The Journal only accepts and publishes those case reports whose learning points provide new insight and/or contribute to advancing medical knowledge both in terms of diagnostics and therapeutic approaches. Case reports of medical errors, therefore, are also welcome as long as they provide innovative measures on how to prevent them in the current practice (Instructive Errors). The Journal may also consider brief and reasoned reports on issues relevant to the practice of Internal Medicine, as well as Abstracts submitted to the scientific meetings of acknowledged medical societies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


