Ko Takamatsu, Chalothorn Wannaphut, Kevin Benavente, Yoshito Nishimura, Christina Chong
{"title":"一个聪明的中风模仿者:没有血吸虫细胞的血栓性血小板减少性紫癜-一例报告和文献综述。","authors":"Ko Takamatsu, Chalothorn Wannaphut, Kevin Benavente, Yoshito Nishimura, Christina Chong","doi":"10.12890/2025_005628","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Thrombotic thrombocytopenic purpura (TTP) is a life-threatening hematologic emergency caused by ADAMTS13 deficiency, leading to microvascular thrombosis, haemolytic anaemia, thrombocytopenia, and end-organ damage. Neurological symptoms occur in up to 90% of cases and are frequently misdiagnosed as stroke. Prompt recognition and treatment reduce the mortality rate from over 90% to 10-20%.</p><p><strong>Case presentation: </strong>A 70-year-old woman with no significant medical history presented with acute aphasia and right-sided facial and upper extremity numbness. Five days prior, she had experienced fatigue, headache, and bruising. On admission, she had stable vitals with mild aphasia and purpuric ecchymoses noted on examination. Laboratory findings revealed haemolytic anaemia (haemoglobin 7.8 g/dl, lactate dehydrogenase 875 U/l, total bilirubin 2.4 mg/dl), thrombocytopenia (35 ×10<sup>9</sup>/l), and unremarkable coagulation studies (partial thromboplastin time 30 sec, prothrombin time-international normalized ratio 1, fibrinogen 370 mg/dl, D-dimer 2.15 ng/ml). Peripheral smear showed no schistocytes but noted 2+spherocytes. Stroke was ruled out with brain magnetic resonance imaging/magnetic resonance angiography. Given the bicytopenia with possible haemolysis along with new neurological symptoms, TTP was considered in the differential diagnosis. A PLASMIC score of 5 suggested a high probability of TTP. Plasma exchange and corticosteroids were initiated within 5 hours of presentation. ADAMTS13 activity <1% confirmed the diagnosis 4 days after presentation. After five plasma exchange sessions, the patient's platelet count normalized and neurologic deficits resolved by discharge.</p><p><strong>Conclusion: </strong>This case underscores the importance of considering TTP in stroke mimics, even in the absence of schistocytes, if clinical suspicion is high. Early recognition and initiation of treatment significantly improve patient outcomes.</p><p><strong>Learning points: </strong>Start plasmapheresis and high-dose steroids immediately for suspected thrombotic thrombocytopenic purpura (TTP), even if schistocytes are absent when clinical suspicions are high.Recognizing TTP's neurological symptoms mimicking stroke is crucial to avoid misdiagnosis and ensure timely treatment.</p>","PeriodicalId":11908,"journal":{"name":"European journal of case reports in internal medicine","volume":"12 9","pages":"005628"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416773/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Clever Stroke Mimic: Thrombotic Thrombocytopenic Purpura Without Schistocytes - A Case Report and Literature Review.\",\"authors\":\"Ko Takamatsu, Chalothorn Wannaphut, Kevin Benavente, Yoshito Nishimura, Christina Chong\",\"doi\":\"10.12890/2025_005628\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Thrombotic thrombocytopenic purpura (TTP) is a life-threatening hematologic emergency caused by ADAMTS13 deficiency, leading to microvascular thrombosis, haemolytic anaemia, thrombocytopenia, and end-organ damage. Neurological symptoms occur in up to 90% of cases and are frequently misdiagnosed as stroke. Prompt recognition and treatment reduce the mortality rate from over 90% to 10-20%.</p><p><strong>Case presentation: </strong>A 70-year-old woman with no significant medical history presented with acute aphasia and right-sided facial and upper extremity numbness. Five days prior, she had experienced fatigue, headache, and bruising. On admission, she had stable vitals with mild aphasia and purpuric ecchymoses noted on examination. Laboratory findings revealed haemolytic anaemia (haemoglobin 7.8 g/dl, lactate dehydrogenase 875 U/l, total bilirubin 2.4 mg/dl), thrombocytopenia (35 ×10<sup>9</sup>/l), and unremarkable coagulation studies (partial thromboplastin time 30 sec, prothrombin time-international normalized ratio 1, fibrinogen 370 mg/dl, D-dimer 2.15 ng/ml). Peripheral smear showed no schistocytes but noted 2+spherocytes. Stroke was ruled out with brain magnetic resonance imaging/magnetic resonance angiography. Given the bicytopenia with possible haemolysis along with new neurological symptoms, TTP was considered in the differential diagnosis. A PLASMIC score of 5 suggested a high probability of TTP. Plasma exchange and corticosteroids were initiated within 5 hours of presentation. ADAMTS13 activity <1% confirmed the diagnosis 4 days after presentation. After five plasma exchange sessions, the patient's platelet count normalized and neurologic deficits resolved by discharge.</p><p><strong>Conclusion: </strong>This case underscores the importance of considering TTP in stroke mimics, even in the absence of schistocytes, if clinical suspicion is high. Early recognition and initiation of treatment significantly improve patient outcomes.</p><p><strong>Learning points: </strong>Start plasmapheresis and high-dose steroids immediately for suspected thrombotic thrombocytopenic purpura (TTP), even if schistocytes are absent when clinical suspicions are high.Recognizing TTP's neurological symptoms mimicking stroke is crucial to avoid misdiagnosis and ensure timely treatment.</p>\",\"PeriodicalId\":11908,\"journal\":{\"name\":\"European journal of case reports in internal medicine\",\"volume\":\"12 9\",\"pages\":\"005628\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416773/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of case reports in internal medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12890/2025_005628\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of case reports in internal medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12890/2025_005628","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:血栓性血小板减少性紫癜(TTP)是由ADAMTS13缺乏引起的危及生命的血液学急症,可导致微血管血栓形成、溶血性贫血、血小板减少和终末器官损伤。高达90%的病例出现神经系统症状,经常被误诊为中风。及时发现和治疗可将死亡率从90%以上降低到10-20%。病例介绍:一名70岁女性,无明显病史,表现为急性失语和右侧面部及上肢麻木。五天前,她感到疲劳、头痛和瘀伤。入院时,患者生命体征稳定,检查发现轻度失语和紫癜性瘀斑。实验室结果显示溶血性贫血(血红蛋白7.8 g/dl,乳酸脱氢酶875 U/l,总胆红素2.4 mg/dl),血小板减少(35 ×109/l),凝血研究不显著(部分凝血活素时间30秒,凝血酶原时间国际标准化比值1,纤维蛋白原370 mg/dl, d -二聚体2.15 ng/ml)。外周涂片未见裂细胞,但见2+球形细胞。脑磁共振成像/磁共振血管造影排除脑卒中。考虑到双氧体减少症可能伴有溶血以及新的神经系统症状,TTP被认为是鉴别诊断的依据。血浆评分为5分提示TTP的可能性很大。在发病5小时内开始血浆置换和皮质类固醇治疗。结论:该病例强调了在卒中模拟中考虑TTP的重要性,即使在没有血吸虫细胞的情况下,如果临床怀疑很高。早期识别和开始治疗可显著改善患者的预后。学习要点:对疑似血栓性血小板减少性紫癜(TTP)立即开始血浆置换和大剂量类固醇,即使在临床怀疑高的情况下没有血吸虫细胞。识别TTP类似中风的神经症状对于避免误诊和确保及时治疗至关重要。
A Clever Stroke Mimic: Thrombotic Thrombocytopenic Purpura Without Schistocytes - A Case Report and Literature Review.
Background: Thrombotic thrombocytopenic purpura (TTP) is a life-threatening hematologic emergency caused by ADAMTS13 deficiency, leading to microvascular thrombosis, haemolytic anaemia, thrombocytopenia, and end-organ damage. Neurological symptoms occur in up to 90% of cases and are frequently misdiagnosed as stroke. Prompt recognition and treatment reduce the mortality rate from over 90% to 10-20%.
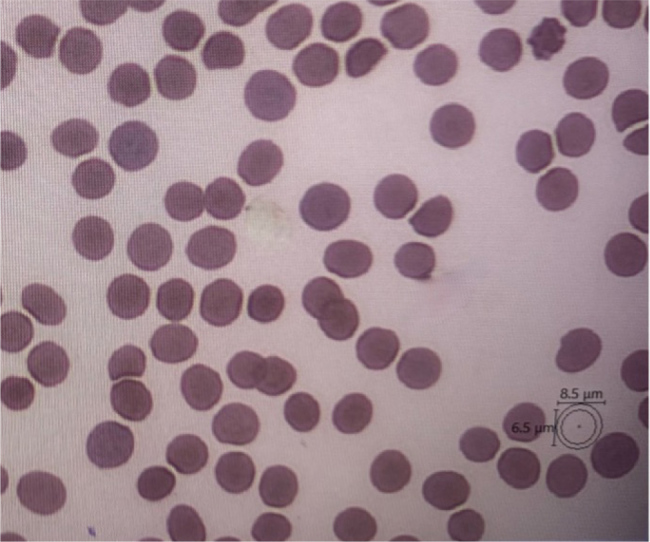
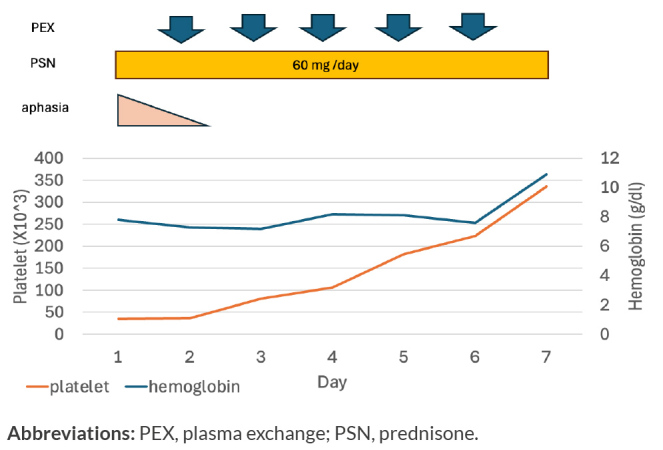
Case presentation: A 70-year-old woman with no significant medical history presented with acute aphasia and right-sided facial and upper extremity numbness. Five days prior, she had experienced fatigue, headache, and bruising. On admission, she had stable vitals with mild aphasia and purpuric ecchymoses noted on examination. Laboratory findings revealed haemolytic anaemia (haemoglobin 7.8 g/dl, lactate dehydrogenase 875 U/l, total bilirubin 2.4 mg/dl), thrombocytopenia (35 ×109/l), and unremarkable coagulation studies (partial thromboplastin time 30 sec, prothrombin time-international normalized ratio 1, fibrinogen 370 mg/dl, D-dimer 2.15 ng/ml). Peripheral smear showed no schistocytes but noted 2+spherocytes. Stroke was ruled out with brain magnetic resonance imaging/magnetic resonance angiography. Given the bicytopenia with possible haemolysis along with new neurological symptoms, TTP was considered in the differential diagnosis. A PLASMIC score of 5 suggested a high probability of TTP. Plasma exchange and corticosteroids were initiated within 5 hours of presentation. ADAMTS13 activity <1% confirmed the diagnosis 4 days after presentation. After five plasma exchange sessions, the patient's platelet count normalized and neurologic deficits resolved by discharge.
Conclusion: This case underscores the importance of considering TTP in stroke mimics, even in the absence of schistocytes, if clinical suspicion is high. Early recognition and initiation of treatment significantly improve patient outcomes.
Learning points: Start plasmapheresis and high-dose steroids immediately for suspected thrombotic thrombocytopenic purpura (TTP), even if schistocytes are absent when clinical suspicions are high.Recognizing TTP's neurological symptoms mimicking stroke is crucial to avoid misdiagnosis and ensure timely treatment.
期刊介绍:
The European Journal of Case Reports in Internal Medicine is an official journal of the European Federation of Internal Medicine (EFIM), representing 35 national societies from 33 European countries. The Journal''s mission is to promote the best medical practice and innovation in the field of acute and general medicine. It also provides a forum for internal medicine doctors where they can share new approaches with the aim of improving diagnostic and clinical skills in this field. EJCRIM welcomes high-quality case reports describing unusual or complex cases that an internist may encounter in everyday practice. The cases should either demonstrate the appropriateness of a diagnostic/therapeutic approach, describe a new procedure or maneuver, or show unusual manifestations of a disease or unexpected reactions. The Journal only accepts and publishes those case reports whose learning points provide new insight and/or contribute to advancing medical knowledge both in terms of diagnostics and therapeutic approaches. Case reports of medical errors, therefore, are also welcome as long as they provide innovative measures on how to prevent them in the current practice (Instructive Errors). The Journal may also consider brief and reasoned reports on issues relevant to the practice of Internal Medicine, as well as Abstracts submitted to the scientific meetings of acknowledged medical societies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


