{"title":"埃塞俄比亚索马里地区吉吉加公立医院5岁以下儿童严重急性营养不良的治疗结果及相关因素:一项回顾性队列研究","authors":"Mustafe Mahamud Abdi, Iid Muktar Jama, Abdilahi Ibrahim Muse, Girma Tadesse Wedajo, Mohamed Omar Osman, Kalkidan Hassen Abate","doi":"10.1136/bmjph-2024-001737","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Severe acute malnutrition (SAM) affects about 20 million under-5 children and contributes to one million child deaths annually. Apart from the presence of clinical management protocols capable of reducing case fatality by 1%-5%, case fatality in hospitals in developing countries averages 20%-30% and has remained the same since the 1950s.</p><p><strong>Objective: </strong>This study aimed to assess treatment outcomes and associated factors of severe acute malnutrition among under-5-year-old children admitted to Jigjiga city public hospitals.</p><p><strong>Methods: </strong>A facility-based retrospective cohort study design was employed on patient records between 1 January 2020 and 31 December, 2021. A structured checklist was used for data extraction to collect data from patient record book. Cox proportional hazards model with a hazard ratio of 95% CI was used. The level of statistical significance was declared at a p<0.05.</p><p><strong>Results: </strong>Overall median length of stay, recovery, death, defaulted and non-responder rate were 7 days, 257 (70.2%), 32 (8.7%), 58 (15.8%) and 19 (5.2%), respectively. Managing facility, tuberculosis (TB), pneumonia and nasogastric (NG) tube insertion were found to be significantly associated with treatment outcomes at a p<0.05.Children who were managed at Jigjiga University Sheik Hassen Yabare Comprehensive Specialised Hospital were 57% less likely to recover from SAM than those managed at Karamardha General Hospital (adjusted hazard ratio (AHR)=0.437, 95% CI: 0.286 to 0.600). Children who did not have TB were almost three times more likely to recover than their counterparts (AHR=2.862, 95% CI: 1.604 to 5.107), and those without pneumonia were also 1.5 times more likely to recover than those with a diagnosis of pneumonia (AHR=1.509, 95% CI: 1.146 to 1.989). Furthermore, children without nasogastric tube insertion were about 1.5 times more likely to recover than their counterparts (AHR=1.472, 95% CI: 1.075 to 2.015).</p><p><strong>Conclusions: </strong>The recovery and defaulter rates fell outside the acceptable targets set by SPHERE standards; however, the death rate was acceptable. The significant predicting factors of treatment outcome were treating facility, TB, pneumonia and NG tube insertion.</p>","PeriodicalId":101362,"journal":{"name":"BMJ public health","volume":"3 2","pages":"e001737"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414189/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatment outcomes and associated factors of severe acute malnutrition among under-5 children in Jigjiga public hospitals, Somali region, Ethiopia: a retrospective cohort study.\",\"authors\":\"Mustafe Mahamud Abdi, Iid Muktar Jama, Abdilahi Ibrahim Muse, Girma Tadesse Wedajo, Mohamed Omar Osman, Kalkidan Hassen Abate\",\"doi\":\"10.1136/bmjph-2024-001737\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Severe acute malnutrition (SAM) affects about 20 million under-5 children and contributes to one million child deaths annually. Apart from the presence of clinical management protocols capable of reducing case fatality by 1%-5%, case fatality in hospitals in developing countries averages 20%-30% and has remained the same since the 1950s.</p><p><strong>Objective: </strong>This study aimed to assess treatment outcomes and associated factors of severe acute malnutrition among under-5-year-old children admitted to Jigjiga city public hospitals.</p><p><strong>Methods: </strong>A facility-based retrospective cohort study design was employed on patient records between 1 January 2020 and 31 December, 2021. A structured checklist was used for data extraction to collect data from patient record book. Cox proportional hazards model with a hazard ratio of 95% CI was used. The level of statistical significance was declared at a p<0.05.</p><p><strong>Results: </strong>Overall median length of stay, recovery, death, defaulted and non-responder rate were 7 days, 257 (70.2%), 32 (8.7%), 58 (15.8%) and 19 (5.2%), respectively. Managing facility, tuberculosis (TB), pneumonia and nasogastric (NG) tube insertion were found to be significantly associated with treatment outcomes at a p<0.05.Children who were managed at Jigjiga University Sheik Hassen Yabare Comprehensive Specialised Hospital were 57% less likely to recover from SAM than those managed at Karamardha General Hospital (adjusted hazard ratio (AHR)=0.437, 95% CI: 0.286 to 0.600). Children who did not have TB were almost three times more likely to recover than their counterparts (AHR=2.862, 95% CI: 1.604 to 5.107), and those without pneumonia were also 1.5 times more likely to recover than those with a diagnosis of pneumonia (AHR=1.509, 95% CI: 1.146 to 1.989). Furthermore, children without nasogastric tube insertion were about 1.5 times more likely to recover than their counterparts (AHR=1.472, 95% CI: 1.075 to 2.015).</p><p><strong>Conclusions: </strong>The recovery and defaulter rates fell outside the acceptable targets set by SPHERE standards; however, the death rate was acceptable. The significant predicting factors of treatment outcome were treating facility, TB, pneumonia and NG tube insertion.</p>\",\"PeriodicalId\":101362,\"journal\":{\"name\":\"BMJ public health\",\"volume\":\"3 2\",\"pages\":\"e001737\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414189/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ public health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjph-2024-001737\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ public health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjph-2024-001737","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Treatment outcomes and associated factors of severe acute malnutrition among under-5 children in Jigjiga public hospitals, Somali region, Ethiopia: a retrospective cohort study.
Background: Severe acute malnutrition (SAM) affects about 20 million under-5 children and contributes to one million child deaths annually. Apart from the presence of clinical management protocols capable of reducing case fatality by 1%-5%, case fatality in hospitals in developing countries averages 20%-30% and has remained the same since the 1950s.
Objective: This study aimed to assess treatment outcomes and associated factors of severe acute malnutrition among under-5-year-old children admitted to Jigjiga city public hospitals.
Methods: A facility-based retrospective cohort study design was employed on patient records between 1 January 2020 and 31 December, 2021. A structured checklist was used for data extraction to collect data from patient record book. Cox proportional hazards model with a hazard ratio of 95% CI was used. The level of statistical significance was declared at a p<0.05.
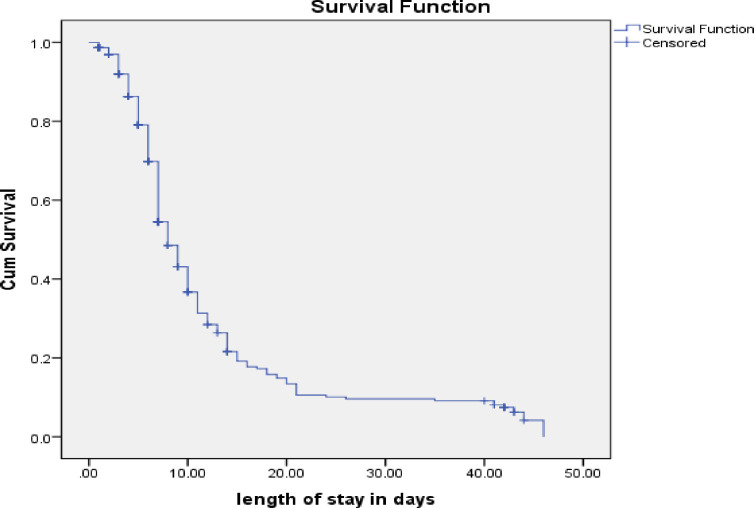
Results: Overall median length of stay, recovery, death, defaulted and non-responder rate were 7 days, 257 (70.2%), 32 (8.7%), 58 (15.8%) and 19 (5.2%), respectively. Managing facility, tuberculosis (TB), pneumonia and nasogastric (NG) tube insertion were found to be significantly associated with treatment outcomes at a p<0.05.Children who were managed at Jigjiga University Sheik Hassen Yabare Comprehensive Specialised Hospital were 57% less likely to recover from SAM than those managed at Karamardha General Hospital (adjusted hazard ratio (AHR)=0.437, 95% CI: 0.286 to 0.600). Children who did not have TB were almost three times more likely to recover than their counterparts (AHR=2.862, 95% CI: 1.604 to 5.107), and those without pneumonia were also 1.5 times more likely to recover than those with a diagnosis of pneumonia (AHR=1.509, 95% CI: 1.146 to 1.989). Furthermore, children without nasogastric tube insertion were about 1.5 times more likely to recover than their counterparts (AHR=1.472, 95% CI: 1.075 to 2.015).
Conclusions: The recovery and defaulter rates fell outside the acceptable targets set by SPHERE standards; however, the death rate was acceptable. The significant predicting factors of treatment outcome were treating facility, TB, pneumonia and NG tube insertion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


