Natália Rocha Tardelli, Fernanda Bono Fukushima, Jenny T van der Steen, Manuel Iván Cobas Rodríguez, Rasa Mikelyte, Daniel Neves Forte, Alex Sander Watanabe Palácio, Vilma Adriana Tripodoro, Mirna Garcia Burgoa, Douglas Henrique Crispim, Alfredo Rodríguez-Núñez, Luis Ricardo González Cruz, Mariuska Forteza Sáez, Patricia Bonilla Sierra, Ancu Tatiana Feng Escobar, María Elena Del Rosario Alcántara Godoy, Tulio Enrique Velásquez Castellanos, Mónica Osio Saldaña, Nisla Camaño Reyes, Miriam Elisa Riveros Ríos, Maria Del Rosario Berenguel Cook, Gloria Castillo Pichardo, Carlos Fernando Acuña Aguilar, Gabriela Píriz Alvarez, Ismariel Inés Espín Gonzalez, Leonardo de Andrade Rodrigues Brito, Edison Iglesias de Oliveira Vidal
{"title":"绘制拉丁美洲的预先护理计划和预先指示。","authors":"Natália Rocha Tardelli, Fernanda Bono Fukushima, Jenny T van der Steen, Manuel Iván Cobas Rodríguez, Rasa Mikelyte, Daniel Neves Forte, Alex Sander Watanabe Palácio, Vilma Adriana Tripodoro, Mirna Garcia Burgoa, Douglas Henrique Crispim, Alfredo Rodríguez-Núñez, Luis Ricardo González Cruz, Mariuska Forteza Sáez, Patricia Bonilla Sierra, Ancu Tatiana Feng Escobar, María Elena Del Rosario Alcántara Godoy, Tulio Enrique Velásquez Castellanos, Mónica Osio Saldaña, Nisla Camaño Reyes, Miriam Elisa Riveros Ríos, Maria Del Rosario Berenguel Cook, Gloria Castillo Pichardo, Carlos Fernando Acuña Aguilar, Gabriela Píriz Alvarez, Ismariel Inés Espín Gonzalez, Leonardo de Andrade Rodrigues Brito, Edison Iglesias de Oliveira Vidal","doi":"10.1186/s12904-025-01849-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aims: </strong>The extent to which low- and middle-income countries have implemented Advance Care Planning (ACP) and Advance Directives (AD) remains unclear. We aimed to map the current status of ACP/AD in Latin America.</p><p><strong>Methods: </strong>This cross-sectional, mixed-methods survey of ACP/AD in LA comprised interviews with 18 key informants from 18 out of 20 countries, most of whom were appointed by national Palliative Care Associations. Online interviews were conducted with each informant, covering a range of relevant topics from AD regulations to the use of ACP/AD in the context of end-of-life clinical decision making. We performed member checking and data triangulation to confirm our findings.</p><p><strong>Results: </strong>Only eight (44%) countries have some form of ACP/AD regulations. Most regulatory frameworks tend to adopt a legalistic pattern heavily influenced by the North American model. Despite that characteristic of AD regulations in LA, the leading strategy used by patients to avoid unwanted treatment at the end of life is through conversations with their families, whereas the least common strategy was consulting with a lawyer. In six (33%) countries, informants believed it was common for patients to grant their families permission to modify their previous choices regarding future treatments. The religiosity/spirituality of populations play an important role in the implementation of ACP in the region. Additionally, respecting patients' preferences of care at the end of life appears to be tied more to aspects related to the characteristics of doctor-patient relationship, and the degree of integration of palliative care into the healthcare system than the existence or content of AD regulations. There was consensus that none of the countries provide sufficient education about ACP/AD to healthcare professionals.</p><p><strong>Conclusions: </strong>Our findings encourage rethinking ACP/AD in LA from a decolonial perspective, considering characteristics such as the preference for a relational model of autonomy in several countries and the importance of taking the religiosity/spirituality of individuals into account during ACP conversations. Our data also suggest that honoring patients' preferences of care at the end of life entails integrating palliative care into health care systems, educating healthcare professionals and the population, and fostering longitudinal trusting relationships between those professionals, patients, and their families.</p>","PeriodicalId":48945,"journal":{"name":"BMC Palliative Care","volume":"24 1","pages":"226"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413744/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mapping advance care planning and advance directives in Latin America.\",\"authors\":\"Natália Rocha Tardelli, Fernanda Bono Fukushima, Jenny T van der Steen, Manuel Iván Cobas Rodríguez, Rasa Mikelyte, Daniel Neves Forte, Alex Sander Watanabe Palácio, Vilma Adriana Tripodoro, Mirna Garcia Burgoa, Douglas Henrique Crispim, Alfredo Rodríguez-Núñez, Luis Ricardo González Cruz, Mariuska Forteza Sáez, Patricia Bonilla Sierra, Ancu Tatiana Feng Escobar, María Elena Del Rosario Alcántara Godoy, Tulio Enrique Velásquez Castellanos, Mónica Osio Saldaña, Nisla Camaño Reyes, Miriam Elisa Riveros Ríos, Maria Del Rosario Berenguel Cook, Gloria Castillo Pichardo, Carlos Fernando Acuña Aguilar, Gabriela Píriz Alvarez, Ismariel Inés Espín Gonzalez, Leonardo de Andrade Rodrigues Brito, Edison Iglesias de Oliveira Vidal\",\"doi\":\"10.1186/s12904-025-01849-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/aims: </strong>The extent to which low- and middle-income countries have implemented Advance Care Planning (ACP) and Advance Directives (AD) remains unclear. We aimed to map the current status of ACP/AD in Latin America.</p><p><strong>Methods: </strong>This cross-sectional, mixed-methods survey of ACP/AD in LA comprised interviews with 18 key informants from 18 out of 20 countries, most of whom were appointed by national Palliative Care Associations. Online interviews were conducted with each informant, covering a range of relevant topics from AD regulations to the use of ACP/AD in the context of end-of-life clinical decision making. We performed member checking and data triangulation to confirm our findings.</p><p><strong>Results: </strong>Only eight (44%) countries have some form of ACP/AD regulations. Most regulatory frameworks tend to adopt a legalistic pattern heavily influenced by the North American model. Despite that characteristic of AD regulations in LA, the leading strategy used by patients to avoid unwanted treatment at the end of life is through conversations with their families, whereas the least common strategy was consulting with a lawyer. In six (33%) countries, informants believed it was common for patients to grant their families permission to modify their previous choices regarding future treatments. The religiosity/spirituality of populations play an important role in the implementation of ACP in the region. Additionally, respecting patients' preferences of care at the end of life appears to be tied more to aspects related to the characteristics of doctor-patient relationship, and the degree of integration of palliative care into the healthcare system than the existence or content of AD regulations. There was consensus that none of the countries provide sufficient education about ACP/AD to healthcare professionals.</p><p><strong>Conclusions: </strong>Our findings encourage rethinking ACP/AD in LA from a decolonial perspective, considering characteristics such as the preference for a relational model of autonomy in several countries and the importance of taking the religiosity/spirituality of individuals into account during ACP conversations. Our data also suggest that honoring patients' preferences of care at the end of life entails integrating palliative care into health care systems, educating healthcare professionals and the population, and fostering longitudinal trusting relationships between those professionals, patients, and their families.</p>\",\"PeriodicalId\":48945,\"journal\":{\"name\":\"BMC Palliative Care\",\"volume\":\"24 1\",\"pages\":\"226\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-09-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413744/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Palliative Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12904-025-01849-5\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Palliative Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12904-025-01849-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Mapping advance care planning and advance directives in Latin America.
Background/aims: The extent to which low- and middle-income countries have implemented Advance Care Planning (ACP) and Advance Directives (AD) remains unclear. We aimed to map the current status of ACP/AD in Latin America.
Methods: This cross-sectional, mixed-methods survey of ACP/AD in LA comprised interviews with 18 key informants from 18 out of 20 countries, most of whom were appointed by national Palliative Care Associations. Online interviews were conducted with each informant, covering a range of relevant topics from AD regulations to the use of ACP/AD in the context of end-of-life clinical decision making. We performed member checking and data triangulation to confirm our findings.
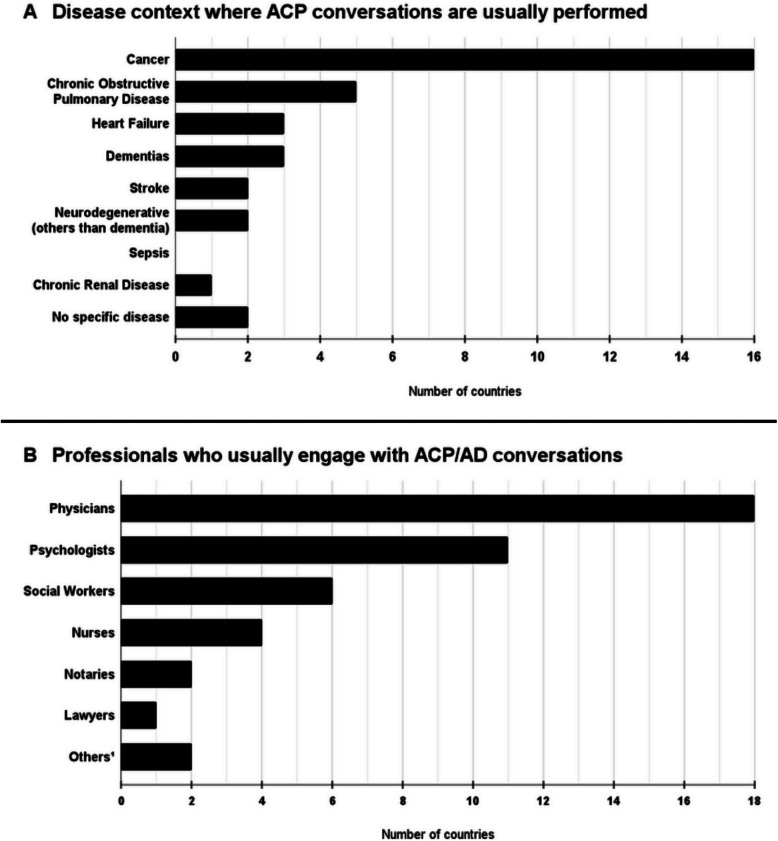
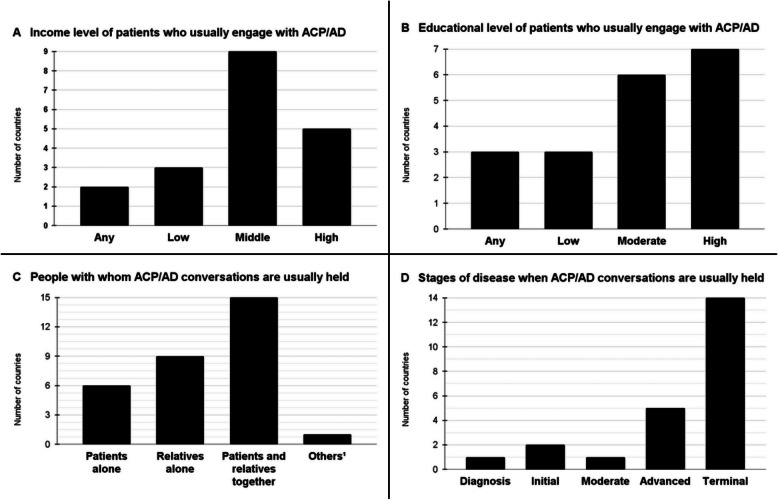
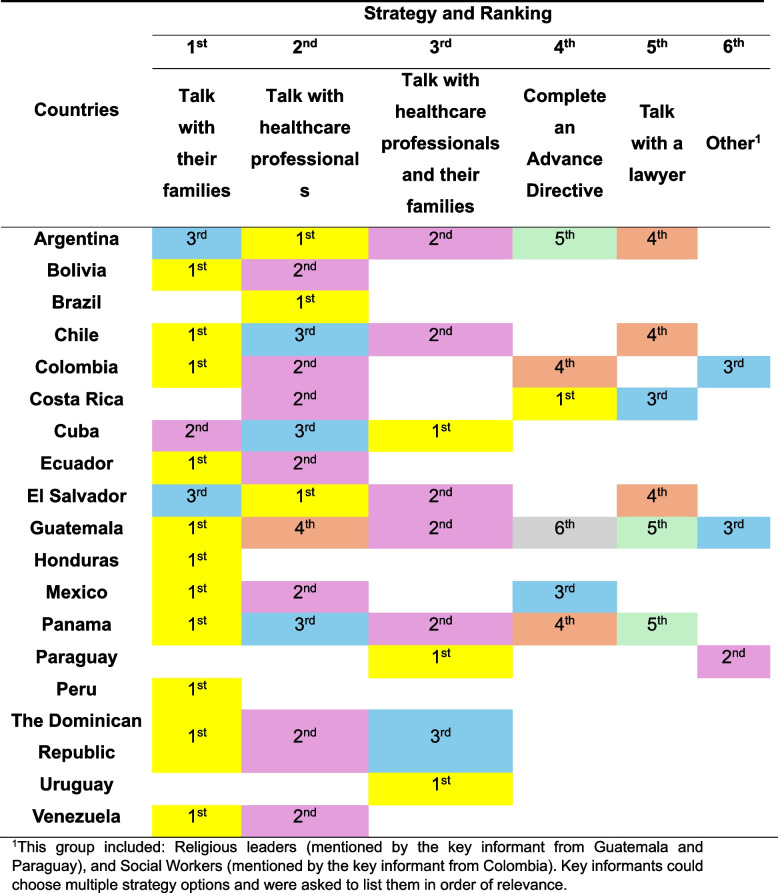
Results: Only eight (44%) countries have some form of ACP/AD regulations. Most regulatory frameworks tend to adopt a legalistic pattern heavily influenced by the North American model. Despite that characteristic of AD regulations in LA, the leading strategy used by patients to avoid unwanted treatment at the end of life is through conversations with their families, whereas the least common strategy was consulting with a lawyer. In six (33%) countries, informants believed it was common for patients to grant their families permission to modify their previous choices regarding future treatments. The religiosity/spirituality of populations play an important role in the implementation of ACP in the region. Additionally, respecting patients' preferences of care at the end of life appears to be tied more to aspects related to the characteristics of doctor-patient relationship, and the degree of integration of palliative care into the healthcare system than the existence or content of AD regulations. There was consensus that none of the countries provide sufficient education about ACP/AD to healthcare professionals.
Conclusions: Our findings encourage rethinking ACP/AD in LA from a decolonial perspective, considering characteristics such as the preference for a relational model of autonomy in several countries and the importance of taking the religiosity/spirituality of individuals into account during ACP conversations. Our data also suggest that honoring patients' preferences of care at the end of life entails integrating palliative care into health care systems, educating healthcare professionals and the population, and fostering longitudinal trusting relationships between those professionals, patients, and their families.
期刊介绍:
BMC Palliative Care is an open access journal publishing original peer-reviewed research articles in the clinical, scientific, ethical and policy issues, local and international, regarding all aspects of hospice and palliative care for the dying and for those with profound suffering related to chronic illness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


