Jordan Herring, Yoon Hong Park, Qian Luo, Anushree Vichare, Clese Erikson, Patricia Pittman
{"title":"医疗补助初级保健利用和地区层面的社会脆弱性。","authors":"Jordan Herring, Yoon Hong Park, Qian Luo, Anushree Vichare, Clese Erikson, Patricia Pittman","doi":"10.1001/jamahealthforum.2025.3020","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The concentration of poverty and multidimensional disadvantage has been shown to limit access to health care in these communities. There is a growing interest in using area-level socioeconomic indexes to address the unequal geographic distribution of health care resources. However, the association of area-level socioeconomic indexes with access to primary care-a key area in health policy-has not been determined.</p><p><strong>Objective: </strong>To investigate the association of Medicaid primary care utilization with the concentration of poverty and multidimensional disadvantage at the zip code level.</p><p><strong>Design, settings, and participants: </strong>This cross-sectional study used the 2019 Transformed-Medicaid Statistical Information System to identify variations in primary care utilization among Medicaid and the Children's Health Insurance Program beneficiaries (age <65 years) by poverty and multidimensional disadvantage levels of their area of residence. Included beneficiaries were enrolled in Medicaid from January 1 to December 31, 2019, and were not dually eligible for Medicare. The zip code-level Social Vulnerability Index (SVI) was used to assess the likelihood of a beneficiary having an annual primary care visit, while controlling for individual beneficiary demographic and health characteristics. An activity-based approach was adopted to classify clinicians billing Medicaid for primary care and to identify primary care visits at federally qualified health centers (FQHCs). SVI results were compared with results using income-based poverty rates alone. Data analysis was performed from May 1, 2023, through February 28, 2025.</p><p><strong>Exposure: </strong>Zip code-level deciles of the SVI and poverty rates.</p><p><strong>Main outcomes and measures: </strong>Regression analysis was performed at the beneficiary level, using a binary indicator for having a primary care visit on a set of dummy variables for SVI deciles, controlling for age and sex interactions, disability status, and indicators for having been diagnosed with behavioral health or chronic physical health conditions.</p><p><strong>Results: </strong>The total population analyzed comprised 34 890 932 Medicaid beneficiaries (<65 years old; 54.2% female and 45.8% male), more than half of whom resided in the top 20% of socially vulnerable zip codes; approximately 33%, in the top 10%; and another 20%, in the ninth decile. Of the total, 68.1% had at least 1 primary care visit in 2019, at either a non-FQHC practice (61.1%) or a FQHC (12.7%). The probability of having a primary care visit was highest for children (age <18 years) but varied substantially by age. Compared to those residing in the first decile of the SVI (least socially vulnerable), beneficiaries in the tenth decile (most socially vulnerable) were 8.9 (95% CI, -9.9 to -7.9) percentage points (pp) less likely to have a primary care visit when not counting FQHC visits, but this increased to 4.7 (95% CI, -5.5 to -3.8) pp less likely when including FQHC visits. Beneficiaries in the tenth decile were 5.9 (95% CI, 4.9 to 6.8) pp more likely to have a FQHC visit than beneficiaries in the first decile. The SVI results identified more beneficiaries with disparities compared to the area-level poverty rate alone.</p><p><strong>Conclusions and relevance: </strong>The findings of this cross-sectional study suggest that Medicaid policy should focus on addressing geography-based disparities in access to care using new measures to target resources. The multidimensional SVI is likely a useful tool to identify small geographic areas with barriers to accessing adequate health care. The FQHC findings suggest that substantially increasing investments and support for FQHCs would address geographic inequities in access to health care.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 9","pages":"e253020"},"PeriodicalIF":11.3000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413652/pdf/","citationCount":"0","resultStr":"{\"title\":\"Medicaid Primary Care Utilization and Area-Level Social Vulnerability.\",\"authors\":\"Jordan Herring, Yoon Hong Park, Qian Luo, Anushree Vichare, Clese Erikson, Patricia Pittman\",\"doi\":\"10.1001/jamahealthforum.2025.3020\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>The concentration of poverty and multidimensional disadvantage has been shown to limit access to health care in these communities. There is a growing interest in using area-level socioeconomic indexes to address the unequal geographic distribution of health care resources. However, the association of area-level socioeconomic indexes with access to primary care-a key area in health policy-has not been determined.</p><p><strong>Objective: </strong>To investigate the association of Medicaid primary care utilization with the concentration of poverty and multidimensional disadvantage at the zip code level.</p><p><strong>Design, settings, and participants: </strong>This cross-sectional study used the 2019 Transformed-Medicaid Statistical Information System to identify variations in primary care utilization among Medicaid and the Children's Health Insurance Program beneficiaries (age <65 years) by poverty and multidimensional disadvantage levels of their area of residence. Included beneficiaries were enrolled in Medicaid from January 1 to December 31, 2019, and were not dually eligible for Medicare. The zip code-level Social Vulnerability Index (SVI) was used to assess the likelihood of a beneficiary having an annual primary care visit, while controlling for individual beneficiary demographic and health characteristics. An activity-based approach was adopted to classify clinicians billing Medicaid for primary care and to identify primary care visits at federally qualified health centers (FQHCs). SVI results were compared with results using income-based poverty rates alone. Data analysis was performed from May 1, 2023, through February 28, 2025.</p><p><strong>Exposure: </strong>Zip code-level deciles of the SVI and poverty rates.</p><p><strong>Main outcomes and measures: </strong>Regression analysis was performed at the beneficiary level, using a binary indicator for having a primary care visit on a set of dummy variables for SVI deciles, controlling for age and sex interactions, disability status, and indicators for having been diagnosed with behavioral health or chronic physical health conditions.</p><p><strong>Results: </strong>The total population analyzed comprised 34 890 932 Medicaid beneficiaries (<65 years old; 54.2% female and 45.8% male), more than half of whom resided in the top 20% of socially vulnerable zip codes; approximately 33%, in the top 10%; and another 20%, in the ninth decile. Of the total, 68.1% had at least 1 primary care visit in 2019, at either a non-FQHC practice (61.1%) or a FQHC (12.7%). The probability of having a primary care visit was highest for children (age <18 years) but varied substantially by age. Compared to those residing in the first decile of the SVI (least socially vulnerable), beneficiaries in the tenth decile (most socially vulnerable) were 8.9 (95% CI, -9.9 to -7.9) percentage points (pp) less likely to have a primary care visit when not counting FQHC visits, but this increased to 4.7 (95% CI, -5.5 to -3.8) pp less likely when including FQHC visits. Beneficiaries in the tenth decile were 5.9 (95% CI, 4.9 to 6.8) pp more likely to have a FQHC visit than beneficiaries in the first decile. The SVI results identified more beneficiaries with disparities compared to the area-level poverty rate alone.</p><p><strong>Conclusions and relevance: </strong>The findings of this cross-sectional study suggest that Medicaid policy should focus on addressing geography-based disparities in access to care using new measures to target resources. The multidimensional SVI is likely a useful tool to identify small geographic areas with barriers to accessing adequate health care. The FQHC findings suggest that substantially increasing investments and support for FQHCs would address geographic inequities in access to health care.</p>\",\"PeriodicalId\":53180,\"journal\":{\"name\":\"JAMA Health Forum\",\"volume\":\"6 9\",\"pages\":\"e253020\"},\"PeriodicalIF\":11.3000,\"publicationDate\":\"2025-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413652/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Health Forum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1001/jamahealthforum.2025.3020\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2025.3020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Medicaid Primary Care Utilization and Area-Level Social Vulnerability.
Importance: The concentration of poverty and multidimensional disadvantage has been shown to limit access to health care in these communities. There is a growing interest in using area-level socioeconomic indexes to address the unequal geographic distribution of health care resources. However, the association of area-level socioeconomic indexes with access to primary care-a key area in health policy-has not been determined.
Objective: To investigate the association of Medicaid primary care utilization with the concentration of poverty and multidimensional disadvantage at the zip code level.
Design, settings, and participants: This cross-sectional study used the 2019 Transformed-Medicaid Statistical Information System to identify variations in primary care utilization among Medicaid and the Children's Health Insurance Program beneficiaries (age <65 years) by poverty and multidimensional disadvantage levels of their area of residence. Included beneficiaries were enrolled in Medicaid from January 1 to December 31, 2019, and were not dually eligible for Medicare. The zip code-level Social Vulnerability Index (SVI) was used to assess the likelihood of a beneficiary having an annual primary care visit, while controlling for individual beneficiary demographic and health characteristics. An activity-based approach was adopted to classify clinicians billing Medicaid for primary care and to identify primary care visits at federally qualified health centers (FQHCs). SVI results were compared with results using income-based poverty rates alone. Data analysis was performed from May 1, 2023, through February 28, 2025.
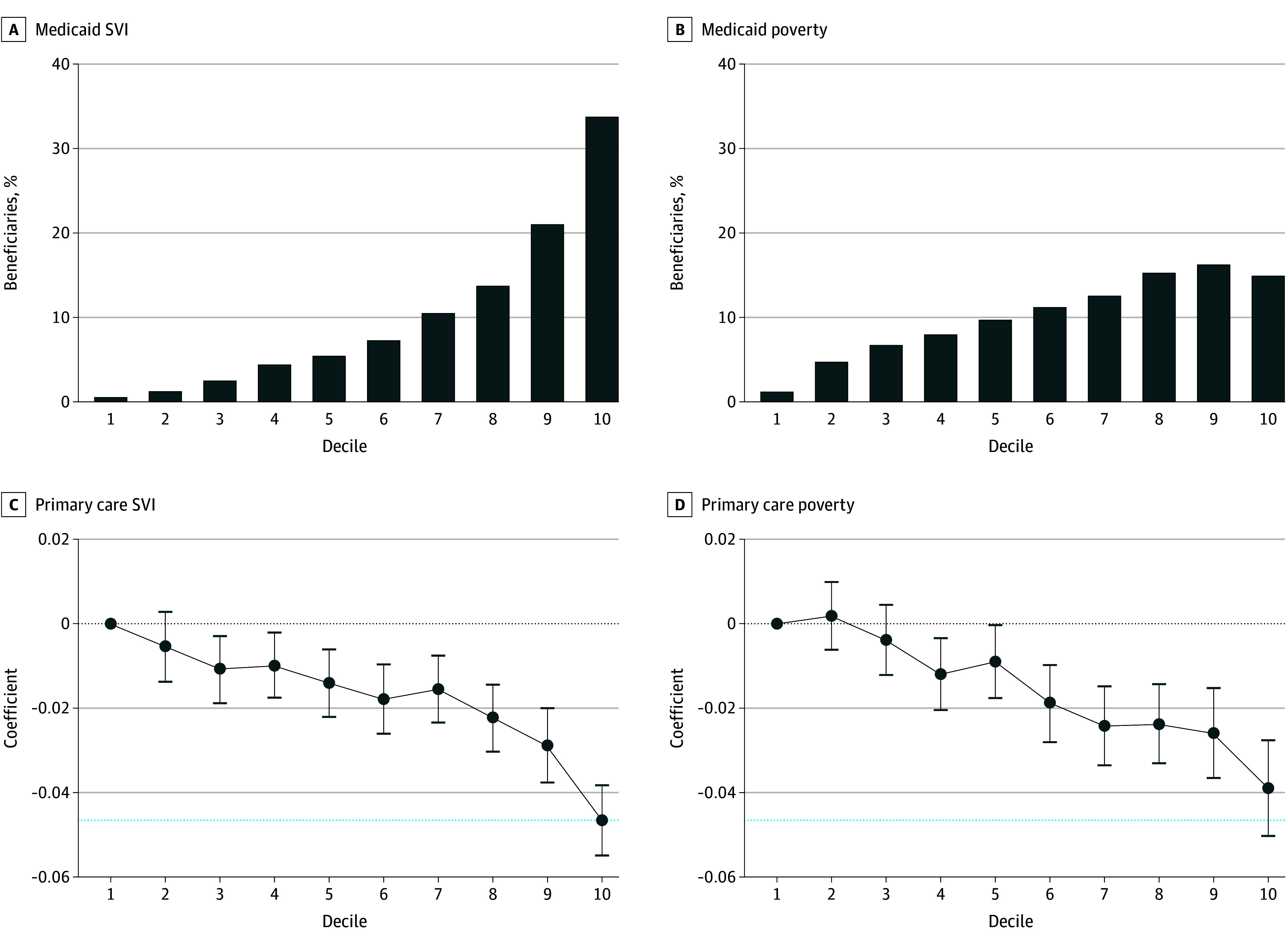
Exposure: Zip code-level deciles of the SVI and poverty rates.
Main outcomes and measures: Regression analysis was performed at the beneficiary level, using a binary indicator for having a primary care visit on a set of dummy variables for SVI deciles, controlling for age and sex interactions, disability status, and indicators for having been diagnosed with behavioral health or chronic physical health conditions.
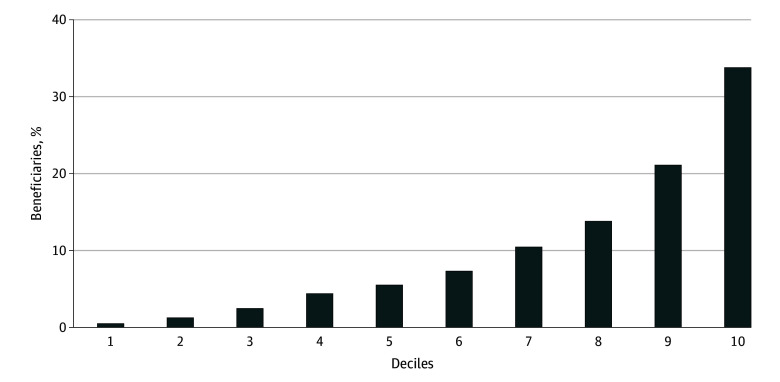
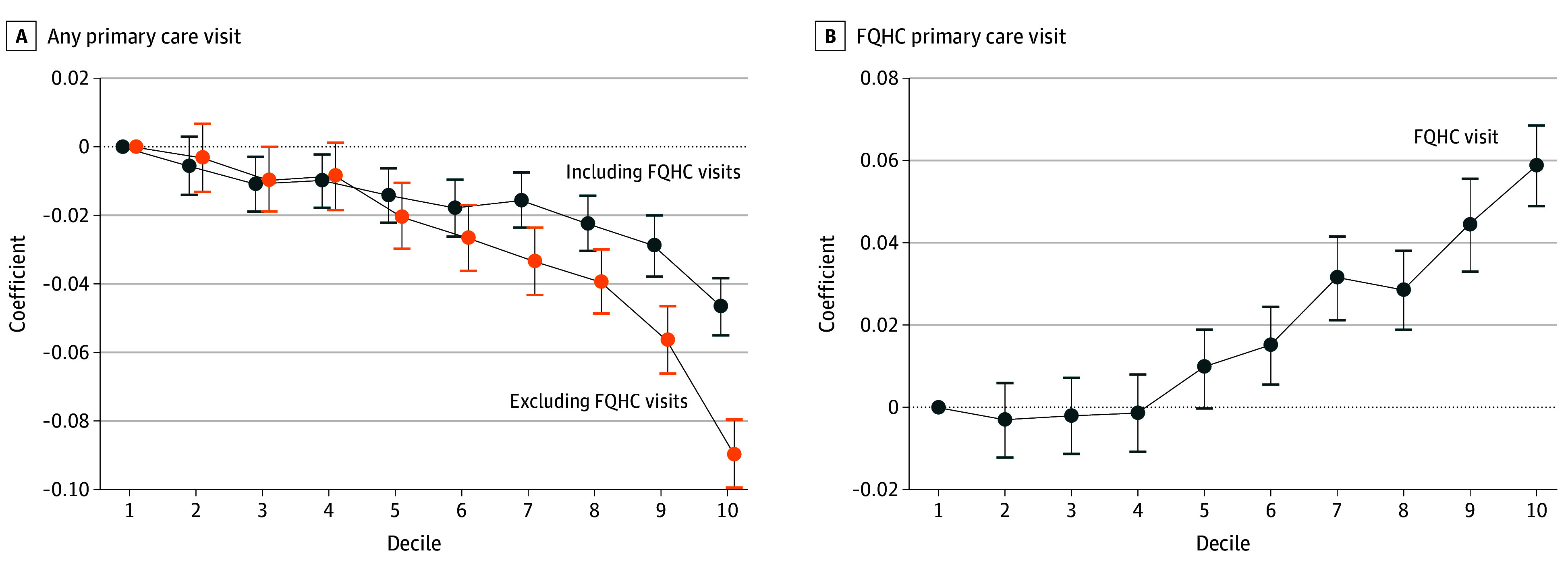
Results: The total population analyzed comprised 34 890 932 Medicaid beneficiaries (<65 years old; 54.2% female and 45.8% male), more than half of whom resided in the top 20% of socially vulnerable zip codes; approximately 33%, in the top 10%; and another 20%, in the ninth decile. Of the total, 68.1% had at least 1 primary care visit in 2019, at either a non-FQHC practice (61.1%) or a FQHC (12.7%). The probability of having a primary care visit was highest for children (age <18 years) but varied substantially by age. Compared to those residing in the first decile of the SVI (least socially vulnerable), beneficiaries in the tenth decile (most socially vulnerable) were 8.9 (95% CI, -9.9 to -7.9) percentage points (pp) less likely to have a primary care visit when not counting FQHC visits, but this increased to 4.7 (95% CI, -5.5 to -3.8) pp less likely when including FQHC visits. Beneficiaries in the tenth decile were 5.9 (95% CI, 4.9 to 6.8) pp more likely to have a FQHC visit than beneficiaries in the first decile. The SVI results identified more beneficiaries with disparities compared to the area-level poverty rate alone.
Conclusions and relevance: The findings of this cross-sectional study suggest that Medicaid policy should focus on addressing geography-based disparities in access to care using new measures to target resources. The multidimensional SVI is likely a useful tool to identify small geographic areas with barriers to accessing adequate health care. The FQHC findings suggest that substantially increasing investments and support for FQHCs would address geographic inequities in access to health care.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


