{"title":"美国医院社会经济贫困地区采用卫生信息技术的情况","authors":"Alice S Yan, Nate C Apathy, Jie Chen","doi":"10.1001/jamahealthforum.2025.3035","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Access to and quality of care vary substantially by area socioeconomic status. Expanding hospital health information technology (HIT) adoption may help reduce these disparities, given hospitals' central role in serving underserved populations.</p><p><strong>Objective: </strong>To examine variations in US hospital adoption of telehealth and health information exchange (HIE) functionalities by hospital service area (HSA) socioeconomic deprivation.</p><p><strong>Design, setting, and participants: </strong>This cross-sectional study links data from the 2018-2023 American Hospital Association Annual Survey and Information Technology Survey with HSA-level area deprivation index. Nonfederal acute care hospitals with complete data on HIT outcomes, comprising 16 646 observations for the telehealth outcomes and 9218 observations for the HIE outcomes across 6 years, were included. Data were analyzed from February 2024 to February 2025.</p><p><strong>Exposures: </strong>HSA-level area deprivation index in quartiles.</p><p><strong>Main outcomes and measures: </strong>Hospital adoption of treatment-stage telehealth and postdischarge telehealth services and HIE infrastructure supporting electronic data query and availability. Descriptive, regression, and Blinder-Oaxaca decomposition analyses and visualized time trends in hospital HIT adoption were used in analyses.</p><p><strong>Results: </strong>This study included 16 646 hospital-level observations and 9218 observations for health information exchange functionalities. Hospitals in the most socioeconomically deprived HSAs were significantly less likely to adopt HIT compared with those in the least deprived areas (treatment-stage telehealth: marginal effect [ME], -0.03; 95% CI, -0.06 to -0.01; postdischarge telehealth: ME, -0.03; 95% CI, -0.07 to 0.01; electronic data query capability: ME, -0.03; 95% CI, -0.06 to -0.01; electronic data availability: ME, -0.06; 95% CI, -0.11 to -0.01). Year fixed effects indicated significant increases in HIT adoption from 2018 to 2023, regardless of HSA deprivation level. Decomposition analyses showed that differences in hospital bed size, urban/rural location, and accountable care organization participation explained a substantial portion of the disparities by HSA deprivation.</p><p><strong>Conclusions and relevance: </strong>In this study, hospitals in more socioeconomically disadvantaged HSAs remained likely to adopt telehealth and HIE functionalities. Nevertheless, HIT adoption has grown steadily over time. Accountable care organization participation may support HIT infrastructure and help reduce geographic disparities in adoption and access to care.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 9","pages":"e253035"},"PeriodicalIF":11.3000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413650/pdf/","citationCount":"0","resultStr":"{\"title\":\"Adoption of Health Information Technologies by Area Socioeconomic Deprivation Among US Hospitals.\",\"authors\":\"Alice S Yan, Nate C Apathy, Jie Chen\",\"doi\":\"10.1001/jamahealthforum.2025.3035\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Access to and quality of care vary substantially by area socioeconomic status. Expanding hospital health information technology (HIT) adoption may help reduce these disparities, given hospitals' central role in serving underserved populations.</p><p><strong>Objective: </strong>To examine variations in US hospital adoption of telehealth and health information exchange (HIE) functionalities by hospital service area (HSA) socioeconomic deprivation.</p><p><strong>Design, setting, and participants: </strong>This cross-sectional study links data from the 2018-2023 American Hospital Association Annual Survey and Information Technology Survey with HSA-level area deprivation index. Nonfederal acute care hospitals with complete data on HIT outcomes, comprising 16 646 observations for the telehealth outcomes and 9218 observations for the HIE outcomes across 6 years, were included. Data were analyzed from February 2024 to February 2025.</p><p><strong>Exposures: </strong>HSA-level area deprivation index in quartiles.</p><p><strong>Main outcomes and measures: </strong>Hospital adoption of treatment-stage telehealth and postdischarge telehealth services and HIE infrastructure supporting electronic data query and availability. Descriptive, regression, and Blinder-Oaxaca decomposition analyses and visualized time trends in hospital HIT adoption were used in analyses.</p><p><strong>Results: </strong>This study included 16 646 hospital-level observations and 9218 observations for health information exchange functionalities. Hospitals in the most socioeconomically deprived HSAs were significantly less likely to adopt HIT compared with those in the least deprived areas (treatment-stage telehealth: marginal effect [ME], -0.03; 95% CI, -0.06 to -0.01; postdischarge telehealth: ME, -0.03; 95% CI, -0.07 to 0.01; electronic data query capability: ME, -0.03; 95% CI, -0.06 to -0.01; electronic data availability: ME, -0.06; 95% CI, -0.11 to -0.01). Year fixed effects indicated significant increases in HIT adoption from 2018 to 2023, regardless of HSA deprivation level. Decomposition analyses showed that differences in hospital bed size, urban/rural location, and accountable care organization participation explained a substantial portion of the disparities by HSA deprivation.</p><p><strong>Conclusions and relevance: </strong>In this study, hospitals in more socioeconomically disadvantaged HSAs remained likely to adopt telehealth and HIE functionalities. Nevertheless, HIT adoption has grown steadily over time. Accountable care organization participation may support HIT infrastructure and help reduce geographic disparities in adoption and access to care.</p>\",\"PeriodicalId\":53180,\"journal\":{\"name\":\"JAMA Health Forum\",\"volume\":\"6 9\",\"pages\":\"e253035\"},\"PeriodicalIF\":11.3000,\"publicationDate\":\"2025-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413650/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Health Forum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1001/jamahealthforum.2025.3035\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2025.3035","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Adoption of Health Information Technologies by Area Socioeconomic Deprivation Among US Hospitals.
Importance: Access to and quality of care vary substantially by area socioeconomic status. Expanding hospital health information technology (HIT) adoption may help reduce these disparities, given hospitals' central role in serving underserved populations.
Objective: To examine variations in US hospital adoption of telehealth and health information exchange (HIE) functionalities by hospital service area (HSA) socioeconomic deprivation.
Design, setting, and participants: This cross-sectional study links data from the 2018-2023 American Hospital Association Annual Survey and Information Technology Survey with HSA-level area deprivation index. Nonfederal acute care hospitals with complete data on HIT outcomes, comprising 16 646 observations for the telehealth outcomes and 9218 observations for the HIE outcomes across 6 years, were included. Data were analyzed from February 2024 to February 2025.
Exposures: HSA-level area deprivation index in quartiles.
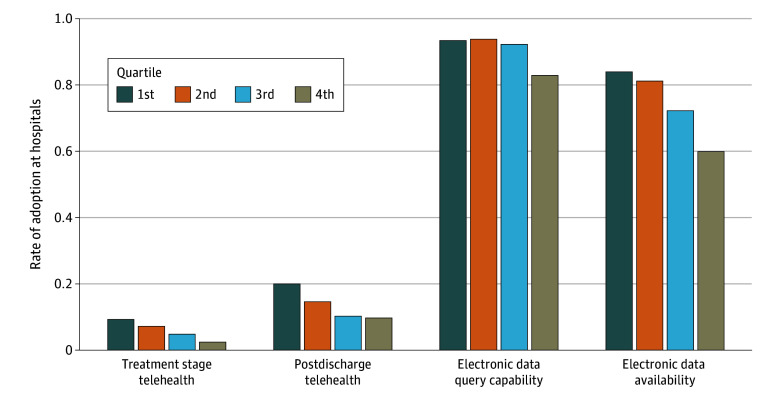
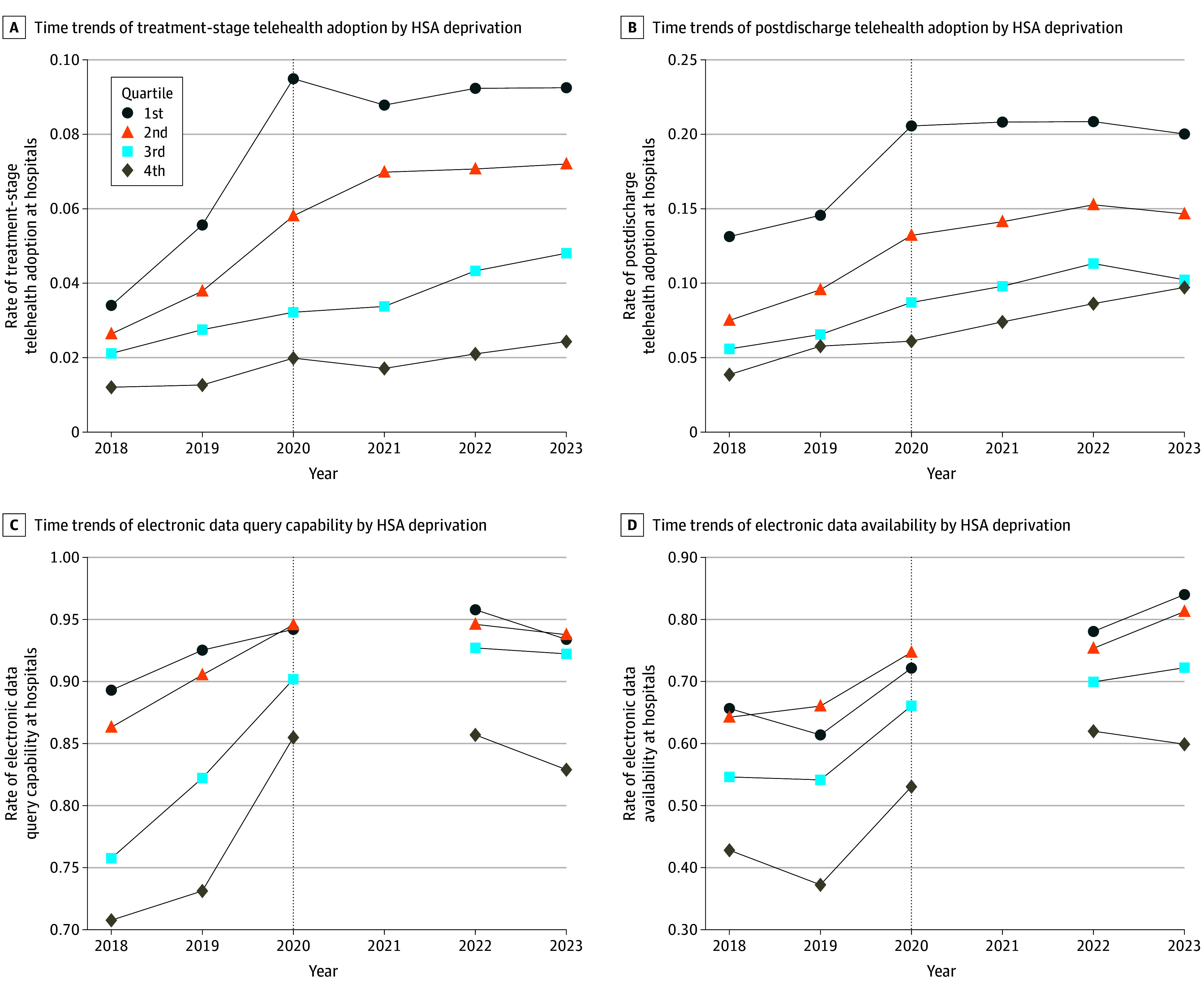
Main outcomes and measures: Hospital adoption of treatment-stage telehealth and postdischarge telehealth services and HIE infrastructure supporting electronic data query and availability. Descriptive, regression, and Blinder-Oaxaca decomposition analyses and visualized time trends in hospital HIT adoption were used in analyses.
Results: This study included 16 646 hospital-level observations and 9218 observations for health information exchange functionalities. Hospitals in the most socioeconomically deprived HSAs were significantly less likely to adopt HIT compared with those in the least deprived areas (treatment-stage telehealth: marginal effect [ME], -0.03; 95% CI, -0.06 to -0.01; postdischarge telehealth: ME, -0.03; 95% CI, -0.07 to 0.01; electronic data query capability: ME, -0.03; 95% CI, -0.06 to -0.01; electronic data availability: ME, -0.06; 95% CI, -0.11 to -0.01). Year fixed effects indicated significant increases in HIT adoption from 2018 to 2023, regardless of HSA deprivation level. Decomposition analyses showed that differences in hospital bed size, urban/rural location, and accountable care organization participation explained a substantial portion of the disparities by HSA deprivation.
Conclusions and relevance: In this study, hospitals in more socioeconomically disadvantaged HSAs remained likely to adopt telehealth and HIE functionalities. Nevertheless, HIT adoption has grown steadily over time. Accountable care organization participation may support HIT infrastructure and help reduce geographic disparities in adoption and access to care.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


