Jongkonnee Chongpornchai, Tuangrat Phodha, Thanawat Wongphan, Kamonwan Soonklang, Peter C Coyte
{"title":"2019冠状病毒病大流行之外:泰国高血压和糖尿病管理远程医疗服务的预算影响分析","authors":"Jongkonnee Chongpornchai, Tuangrat Phodha, Thanawat Wongphan, Kamonwan Soonklang, Peter C Coyte","doi":"10.2147/CEOR.S538395","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The COVID-19 pandemic disrupted healthcare services globally, necessitating innovative care delivery models for non-communicable diseases. Remote healthcare pathways, including telehealth with pharmacy at home (PAH) and deferred care (DC), emerged as potential solutions for managing stable hypertension (HT) and diabetes mellitus (DM) patients. This study aims to estimate the budget impact of implementing PAH and DC compared to usual care (UC) for HT and DM patients in Thai tertiary care hospitals from the government perspective.</p><p><strong>Methods: </strong> A retrospective budget impact analysis was conducted using data from July-December 2021 (COVID-19 period) and July-December 2022 (new normal period). The study included stable patients from 35 tertiary care hospitals in Thailand. Direct medical costs were obtained from administrative databases and national costing studies. Multivariate log-linear regression models estimated conditional costs, controlling for patient characteristics. The analysis compared baseline scenario (UC only) versus alternative scenario (UC+PAH+DC). Sensitivity analyses were performed using 95% confidence intervals and ±20% population variations.</p><p><strong>Results: </strong> The alternative scenario demonstrated lower total budgets in both periods. During COVID-19, total costs were 12.23 versus 12.94 million USD (baseline), yielding 0.71 million USD in savings. In the new normal, costs were 11.93 versus 12.54 million USD (baseline), generating 0.61 million USD in savings. Cost-saving ratios were 0.06 USD and 0.05 USD per dollar allocated during the COVID-19 and new normal periods, respectively. Sensitivity analyses confirmed robustness across parameter variations.</p><p><strong>Conclusion: </strong>PAH and DC pathways represent economically advantageous alternatives, demonstrating cost savings from the government perspective. These findings support implementing remote healthcare delivery in resource-constrained settings, though comprehensive evaluations incorporating societal and patient perspectives are warranted. The findings are based on extrapolation-based results and should be interpreted with caution due to variability in parameters including adoption rates of PAH/DC, unit costs applied, patient numbers, retrospective design, bundled interventions, and the savings ratio.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"627-638"},"PeriodicalIF":2.2000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406030/pdf/","citationCount":"0","resultStr":"{\"title\":\"Beyond the COVID-19 Pandemic: Budget Impact Analysis of Remote Healthcare Delivery for Hypertension and Diabetes Mellitus Management in Thailand.\",\"authors\":\"Jongkonnee Chongpornchai, Tuangrat Phodha, Thanawat Wongphan, Kamonwan Soonklang, Peter C Coyte\",\"doi\":\"10.2147/CEOR.S538395\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The COVID-19 pandemic disrupted healthcare services globally, necessitating innovative care delivery models for non-communicable diseases. Remote healthcare pathways, including telehealth with pharmacy at home (PAH) and deferred care (DC), emerged as potential solutions for managing stable hypertension (HT) and diabetes mellitus (DM) patients. This study aims to estimate the budget impact of implementing PAH and DC compared to usual care (UC) for HT and DM patients in Thai tertiary care hospitals from the government perspective.</p><p><strong>Methods: </strong> A retrospective budget impact analysis was conducted using data from July-December 2021 (COVID-19 period) and July-December 2022 (new normal period). The study included stable patients from 35 tertiary care hospitals in Thailand. Direct medical costs were obtained from administrative databases and national costing studies. Multivariate log-linear regression models estimated conditional costs, controlling for patient characteristics. The analysis compared baseline scenario (UC only) versus alternative scenario (UC+PAH+DC). Sensitivity analyses were performed using 95% confidence intervals and ±20% population variations.</p><p><strong>Results: </strong> The alternative scenario demonstrated lower total budgets in both periods. During COVID-19, total costs were 12.23 versus 12.94 million USD (baseline), yielding 0.71 million USD in savings. In the new normal, costs were 11.93 versus 12.54 million USD (baseline), generating 0.61 million USD in savings. Cost-saving ratios were 0.06 USD and 0.05 USD per dollar allocated during the COVID-19 and new normal periods, respectively. Sensitivity analyses confirmed robustness across parameter variations.</p><p><strong>Conclusion: </strong>PAH and DC pathways represent economically advantageous alternatives, demonstrating cost savings from the government perspective. These findings support implementing remote healthcare delivery in resource-constrained settings, though comprehensive evaluations incorporating societal and patient perspectives are warranted. The findings are based on extrapolation-based results and should be interpreted with caution due to variability in parameters including adoption rates of PAH/DC, unit costs applied, patient numbers, retrospective design, bundled interventions, and the savings ratio.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"17 \",\"pages\":\"627-638\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406030/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S538395\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S538395","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Beyond the COVID-19 Pandemic: Budget Impact Analysis of Remote Healthcare Delivery for Hypertension and Diabetes Mellitus Management in Thailand.
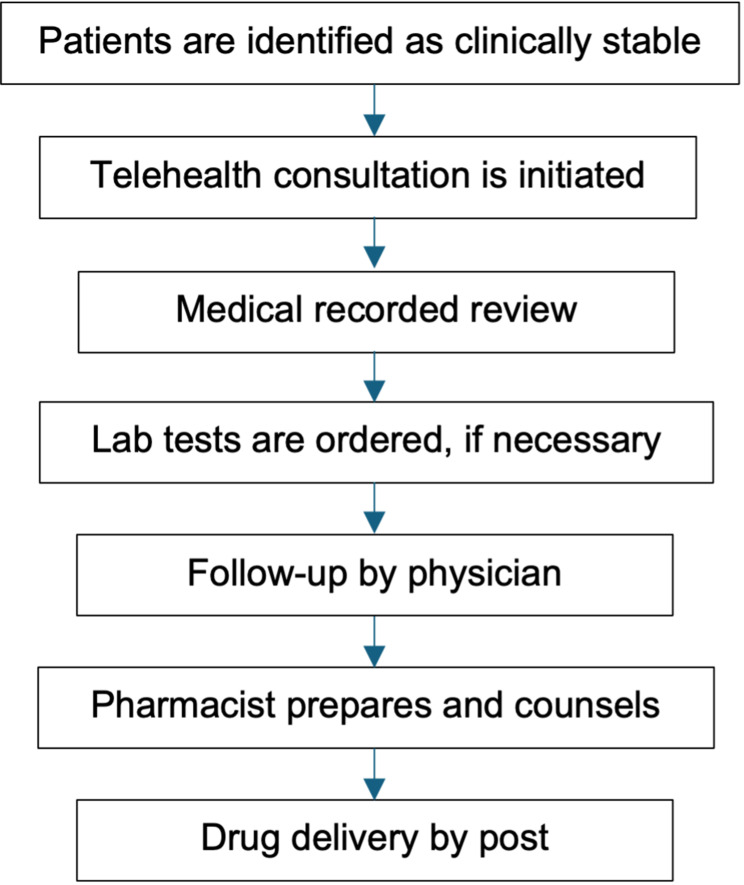
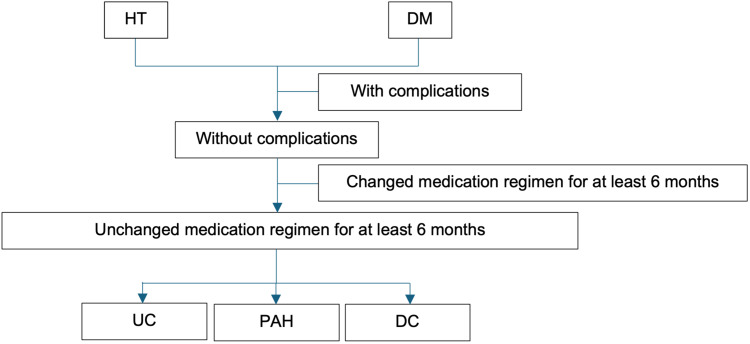
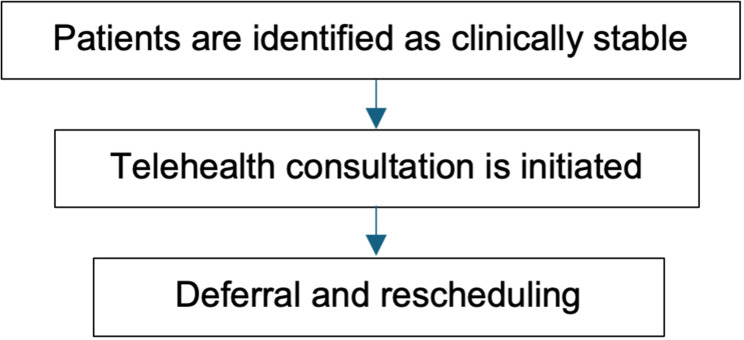
Purpose: The COVID-19 pandemic disrupted healthcare services globally, necessitating innovative care delivery models for non-communicable diseases. Remote healthcare pathways, including telehealth with pharmacy at home (PAH) and deferred care (DC), emerged as potential solutions for managing stable hypertension (HT) and diabetes mellitus (DM) patients. This study aims to estimate the budget impact of implementing PAH and DC compared to usual care (UC) for HT and DM patients in Thai tertiary care hospitals from the government perspective.
Methods: A retrospective budget impact analysis was conducted using data from July-December 2021 (COVID-19 period) and July-December 2022 (new normal period). The study included stable patients from 35 tertiary care hospitals in Thailand. Direct medical costs were obtained from administrative databases and national costing studies. Multivariate log-linear regression models estimated conditional costs, controlling for patient characteristics. The analysis compared baseline scenario (UC only) versus alternative scenario (UC+PAH+DC). Sensitivity analyses were performed using 95% confidence intervals and ±20% population variations.
Results: The alternative scenario demonstrated lower total budgets in both periods. During COVID-19, total costs were 12.23 versus 12.94 million USD (baseline), yielding 0.71 million USD in savings. In the new normal, costs were 11.93 versus 12.54 million USD (baseline), generating 0.61 million USD in savings. Cost-saving ratios were 0.06 USD and 0.05 USD per dollar allocated during the COVID-19 and new normal periods, respectively. Sensitivity analyses confirmed robustness across parameter variations.
Conclusion: PAH and DC pathways represent economically advantageous alternatives, demonstrating cost savings from the government perspective. These findings support implementing remote healthcare delivery in resource-constrained settings, though comprehensive evaluations incorporating societal and patient perspectives are warranted. The findings are based on extrapolation-based results and should be interpreted with caution due to variability in parameters including adoption rates of PAH/DC, unit costs applied, patient numbers, retrospective design, bundled interventions, and the savings ratio.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


