Juan F Gallegos-Orozco, Jacqueline G O'Leary, Kapuluru Gautham Reddy, Jas Bindra, Ishveen Chopra, John Niewoehner, Xingyue Huang
{"title":"早期诊断和及时使用特利加压素治疗肝肾综合征可改善预期预后并降低成本。","authors":"Juan F Gallegos-Orozco, Jacqueline G O'Leary, Kapuluru Gautham Reddy, Jas Bindra, Ishveen Chopra, John Niewoehner, Xingyue Huang","doi":"10.2147/CEOR.S530832","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Terlipressin is the only Food and Drug Administration-approved medication for adults with hepatorenal syndrome-acute kidney injury (HRS-AKI) with rapid reduction in kidney function. Treatment with terlipressin, particularly in patients with lower serum creatinine (SCr) at diagnosis, improves outcomes. Despite evidence suggesting that treating HRS-AKI at lower SCr thresholds may improve clinical outcomes, the impact on healthcare resource utilization (HCRU) and medical costs of an earlier intervention strategy remains unquantified. This model-based analysis was conducted from a United States hospital perspective to project the clinical and economic impact of early HRS-AKI diagnosis and treatment with terlipressin among adults.</p><p><strong>Methods: </strong>A decision-analytic model compared two SCr level-based scenarios and projected the outcomes for both scenarios. For current clinical practice, patient distribution was based on the CONFIRM trial (SCr <3 mg/dL: 45% and ≥3 to <5 mg/dL: 55%). For early diagnosis and treatment, distribution was based on the HRS medical chart review study (<3 mg/dL: 85% and ≥3 to <5 mg/dL: 15%). Terlipressin HRS reversal rate for the on-label population (SCr <5 mg/dL and acute-on-chronic liver failure grade 0-2) was 52.2% for SCr <3 mg/dL and 33.3% for SCr ≥3 to <5 mg/dL. An annual HRS incidence of 50,000 was assumed.</p><p><strong>Results: </strong>Based on the modeled projections, early diagnosis and treatment with terlipressin versus current practice yielded an additional 3040 HRS reversals and consequently led to a reduction in hospital days and intensive care unit days. Early intervention resulted in 960 fewer patients requiring renal replacement therapy during hospitalization and 1200 more patients with 90-day transplant-free survival. Early intervention is projected to save $11,504 per patient, with total national savings of $460.2 million annually.</p><p><strong>Conclusion: </strong>Based on the modeled projections using data from clinical trial, earlier HRS diagnosis and treatment with terlipressin may improve clinical outcomes, reduce HCRU, and save costs versus current clinical practice.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"615-625"},"PeriodicalIF":2.2000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404205/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early Diagnosis and Timely Terlipressin in Hepatorenal Syndrome Improves Projected Outcomes and Lowers Cost.\",\"authors\":\"Juan F Gallegos-Orozco, Jacqueline G O'Leary, Kapuluru Gautham Reddy, Jas Bindra, Ishveen Chopra, John Niewoehner, Xingyue Huang\",\"doi\":\"10.2147/CEOR.S530832\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Terlipressin is the only Food and Drug Administration-approved medication for adults with hepatorenal syndrome-acute kidney injury (HRS-AKI) with rapid reduction in kidney function. Treatment with terlipressin, particularly in patients with lower serum creatinine (SCr) at diagnosis, improves outcomes. Despite evidence suggesting that treating HRS-AKI at lower SCr thresholds may improve clinical outcomes, the impact on healthcare resource utilization (HCRU) and medical costs of an earlier intervention strategy remains unquantified. This model-based analysis was conducted from a United States hospital perspective to project the clinical and economic impact of early HRS-AKI diagnosis and treatment with terlipressin among adults.</p><p><strong>Methods: </strong>A decision-analytic model compared two SCr level-based scenarios and projected the outcomes for both scenarios. For current clinical practice, patient distribution was based on the CONFIRM trial (SCr <3 mg/dL: 45% and ≥3 to <5 mg/dL: 55%). For early diagnosis and treatment, distribution was based on the HRS medical chart review study (<3 mg/dL: 85% and ≥3 to <5 mg/dL: 15%). Terlipressin HRS reversal rate for the on-label population (SCr <5 mg/dL and acute-on-chronic liver failure grade 0-2) was 52.2% for SCr <3 mg/dL and 33.3% for SCr ≥3 to <5 mg/dL. An annual HRS incidence of 50,000 was assumed.</p><p><strong>Results: </strong>Based on the modeled projections, early diagnosis and treatment with terlipressin versus current practice yielded an additional 3040 HRS reversals and consequently led to a reduction in hospital days and intensive care unit days. Early intervention resulted in 960 fewer patients requiring renal replacement therapy during hospitalization and 1200 more patients with 90-day transplant-free survival. Early intervention is projected to save $11,504 per patient, with total national savings of $460.2 million annually.</p><p><strong>Conclusion: </strong>Based on the modeled projections using data from clinical trial, earlier HRS diagnosis and treatment with terlipressin may improve clinical outcomes, reduce HCRU, and save costs versus current clinical practice.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"17 \",\"pages\":\"615-625\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404205/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S530832\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S530832","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Early Diagnosis and Timely Terlipressin in Hepatorenal Syndrome Improves Projected Outcomes and Lowers Cost.
Introduction: Terlipressin is the only Food and Drug Administration-approved medication for adults with hepatorenal syndrome-acute kidney injury (HRS-AKI) with rapid reduction in kidney function. Treatment with terlipressin, particularly in patients with lower serum creatinine (SCr) at diagnosis, improves outcomes. Despite evidence suggesting that treating HRS-AKI at lower SCr thresholds may improve clinical outcomes, the impact on healthcare resource utilization (HCRU) and medical costs of an earlier intervention strategy remains unquantified. This model-based analysis was conducted from a United States hospital perspective to project the clinical and economic impact of early HRS-AKI diagnosis and treatment with terlipressin among adults.
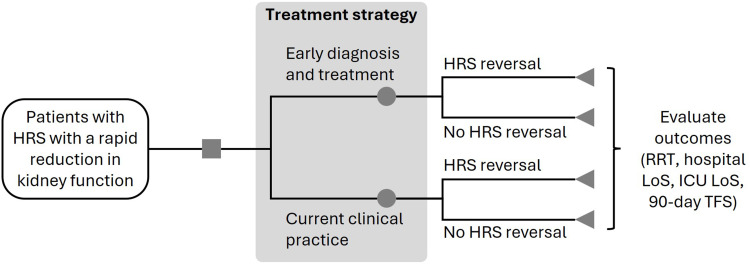
Methods: A decision-analytic model compared two SCr level-based scenarios and projected the outcomes for both scenarios. For current clinical practice, patient distribution was based on the CONFIRM trial (SCr <3 mg/dL: 45% and ≥3 to <5 mg/dL: 55%). For early diagnosis and treatment, distribution was based on the HRS medical chart review study (<3 mg/dL: 85% and ≥3 to <5 mg/dL: 15%). Terlipressin HRS reversal rate for the on-label population (SCr <5 mg/dL and acute-on-chronic liver failure grade 0-2) was 52.2% for SCr <3 mg/dL and 33.3% for SCr ≥3 to <5 mg/dL. An annual HRS incidence of 50,000 was assumed.
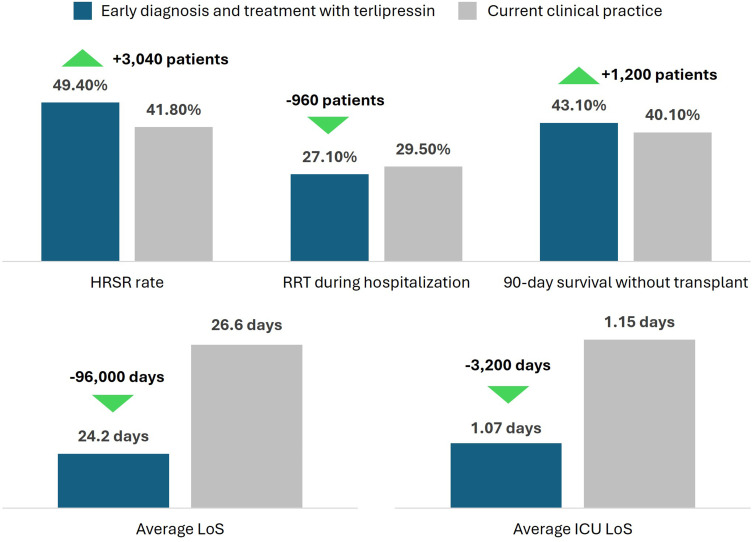
Results: Based on the modeled projections, early diagnosis and treatment with terlipressin versus current practice yielded an additional 3040 HRS reversals and consequently led to a reduction in hospital days and intensive care unit days. Early intervention resulted in 960 fewer patients requiring renal replacement therapy during hospitalization and 1200 more patients with 90-day transplant-free survival. Early intervention is projected to save $11,504 per patient, with total national savings of $460.2 million annually.
Conclusion: Based on the modeled projections using data from clinical trial, earlier HRS diagnosis and treatment with terlipressin may improve clinical outcomes, reduce HCRU, and save costs versus current clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


