{"title":"基于双参数磁共振成像的放射学和深度学习模型预测肝细胞癌Ki-67危险分层。","authors":"Xue-Yong Zuo, Hai-Feng Liu","doi":"10.4254/wjh.v17.i8.109530","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepatocellular carcinoma (HCC) is a prevalent and life-threatening cancer with increasing incidence worldwide. High Ki-67 risk stratification is closely associated with higher recurrence rates and worse outcomes following curative therapies in patients with HCC. However, the performance of radiomic and deep transfer learning (DTL) models derived from biparametric magnetic resonance imaging (bpMRI) in predicting Ki-67 risk stratification and recurrence-free survival (RFS) in patients with HCC remains limited.</p><p><strong>Aim: </strong>To develop a nomogram model integrating bpMRI-based radiomic and DTL signatures for predicting Ki-67 risk stratification and RFS in patients with HCC.</p><p><strong>Methods: </strong>This study included 198 patients with histopathologically confirmed HCC who underwent preoperative bpMRI. Ki-67 risk stratification was categorized as high (> 20%) or low (≤ 20%) according to immunohistochemical staining. Radiomic and DTL signatures were extracted from the T2-weighted and arterial-phase images and combined through a random forest algorithm to establish radiomic and DTL models, respectively. Multivariate regression analysis identified clinical risk factors for high Ki-67 risk stratification, and a predictive nomogram model was developed.</p><p><strong>Results: </strong>A nonsmooth margin and the absence of an enhanced capsule were independent factors for high Ki-67 risk stratification. The area under the curve (AUC) of the clinical model was 0.77, while those of the radiomic and DTL models were 0.81 and 0.87, respectively, for the prediction of high Ki-67 risk stratification, and the nomogram model achieved a better AUC of 0.92. The median RFS times for patients with high and low Ki-67 risk stratification were 33.00 months and 66.73 months, respectively (<i>P</i> < 0.001). Additionally, patients who were predicted to have high Ki-67 risk stratification by the nomogram model had a lower median RFS than those who were predicted to have low Ki-67 risk stratification (33.53 <i>vs</i> 66.74 months, <i>P</i> = 0.007).</p><p><strong>Conclusion: </strong>Our developed nomogram model demonstrated good performance in predicting Ki-67 risk stratification and predicting survival outcomes in patients with HCC.</p>","PeriodicalId":23687,"journal":{"name":"World Journal of Hepatology","volume":"17 8","pages":"109530"},"PeriodicalIF":2.5000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400337/pdf/","citationCount":"0","resultStr":"{\"title\":\"Biparametric magnetic resonance imaging-based radiomic and deep learning models for predicting Ki-67 risk stratification in hepatocellular carcinoma.\",\"authors\":\"Xue-Yong Zuo, Hai-Feng Liu\",\"doi\":\"10.4254/wjh.v17.i8.109530\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hepatocellular carcinoma (HCC) is a prevalent and life-threatening cancer with increasing incidence worldwide. High Ki-67 risk stratification is closely associated with higher recurrence rates and worse outcomes following curative therapies in patients with HCC. However, the performance of radiomic and deep transfer learning (DTL) models derived from biparametric magnetic resonance imaging (bpMRI) in predicting Ki-67 risk stratification and recurrence-free survival (RFS) in patients with HCC remains limited.</p><p><strong>Aim: </strong>To develop a nomogram model integrating bpMRI-based radiomic and DTL signatures for predicting Ki-67 risk stratification and RFS in patients with HCC.</p><p><strong>Methods: </strong>This study included 198 patients with histopathologically confirmed HCC who underwent preoperative bpMRI. Ki-67 risk stratification was categorized as high (> 20%) or low (≤ 20%) according to immunohistochemical staining. Radiomic and DTL signatures were extracted from the T2-weighted and arterial-phase images and combined through a random forest algorithm to establish radiomic and DTL models, respectively. Multivariate regression analysis identified clinical risk factors for high Ki-67 risk stratification, and a predictive nomogram model was developed.</p><p><strong>Results: </strong>A nonsmooth margin and the absence of an enhanced capsule were independent factors for high Ki-67 risk stratification. The area under the curve (AUC) of the clinical model was 0.77, while those of the radiomic and DTL models were 0.81 and 0.87, respectively, for the prediction of high Ki-67 risk stratification, and the nomogram model achieved a better AUC of 0.92. The median RFS times for patients with high and low Ki-67 risk stratification were 33.00 months and 66.73 months, respectively (<i>P</i> < 0.001). Additionally, patients who were predicted to have high Ki-67 risk stratification by the nomogram model had a lower median RFS than those who were predicted to have low Ki-67 risk stratification (33.53 <i>vs</i> 66.74 months, <i>P</i> = 0.007).</p><p><strong>Conclusion: </strong>Our developed nomogram model demonstrated good performance in predicting Ki-67 risk stratification and predicting survival outcomes in patients with HCC.</p>\",\"PeriodicalId\":23687,\"journal\":{\"name\":\"World Journal of Hepatology\",\"volume\":\"17 8\",\"pages\":\"109530\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400337/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Hepatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4254/wjh.v17.i8.109530\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4254/wjh.v17.i8.109530","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
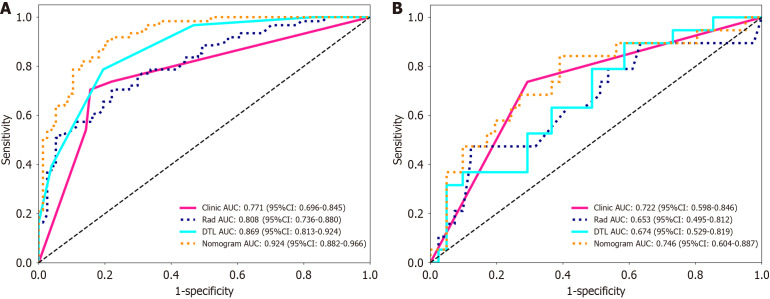
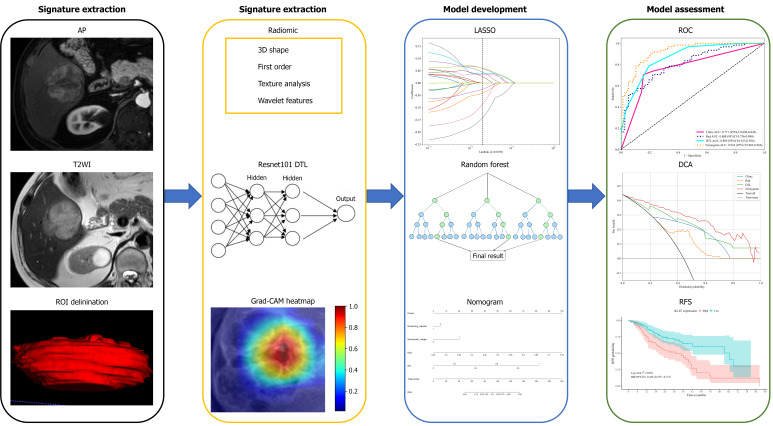
背景:肝细胞癌(HCC)是一种普遍存在的危及生命的癌症,其发病率在世界范围内呈上升趋势。高Ki-67风险分层与HCC患者高复发率和治疗后较差的预后密切相关。然而,基于双参数磁共振成像(bpMRI)的放射学和深度转移学习(DTL)模型在预测HCC患者Ki-67风险分层和无复发生存(RFS)方面的表现仍然有限。目的:建立一种结合基于bpmri的放射学和DTL特征的nomogram模型,用于预测HCC患者的Ki-67风险分层和RFS。方法:本研究纳入198例经组织病理学证实的HCC患者,术前行bpMRI检查。根据免疫组化染色将Ki-67危险分层分为高(≤20%)和低(≤20%)。从t2加权和动脉期图像中提取Radiomic和DTL特征,并通过随机森林算法组合,分别建立Radiomic和DTL模型。多因素回归分析确定Ki-67高危分层的临床危险因素,并建立预测nomogram模型。结果:边缘不光滑和没有增强包膜是Ki-67高危分层的独立因素。临床模型预测Ki-67高危险分层的曲线下面积(AUC)为0.77,放射组学模型和DTL模型的AUC分别为0.81和0.87,其中nomogram模型的AUC为0.92。高、低Ki-67危险分层患者的中位RFS时间分别为33.00个月和66.73个月(P < 0.001)。此外,通过nomogram模型预测Ki-67风险分层较高的患者的中位RFS低于预测Ki-67风险分层较低的患者(33.53 vs 66.74个月,P = 0.007)。结论:我们开发的nomogram模型在预测HCC患者Ki-67风险分层和预测生存结局方面表现良好。
Biparametric magnetic resonance imaging-based radiomic and deep learning models for predicting Ki-67 risk stratification in hepatocellular carcinoma.
Background: Hepatocellular carcinoma (HCC) is a prevalent and life-threatening cancer with increasing incidence worldwide. High Ki-67 risk stratification is closely associated with higher recurrence rates and worse outcomes following curative therapies in patients with HCC. However, the performance of radiomic and deep transfer learning (DTL) models derived from biparametric magnetic resonance imaging (bpMRI) in predicting Ki-67 risk stratification and recurrence-free survival (RFS) in patients with HCC remains limited.
Aim: To develop a nomogram model integrating bpMRI-based radiomic and DTL signatures for predicting Ki-67 risk stratification and RFS in patients with HCC.
Methods: This study included 198 patients with histopathologically confirmed HCC who underwent preoperative bpMRI. Ki-67 risk stratification was categorized as high (> 20%) or low (≤ 20%) according to immunohistochemical staining. Radiomic and DTL signatures were extracted from the T2-weighted and arterial-phase images and combined through a random forest algorithm to establish radiomic and DTL models, respectively. Multivariate regression analysis identified clinical risk factors for high Ki-67 risk stratification, and a predictive nomogram model was developed.
Results: A nonsmooth margin and the absence of an enhanced capsule were independent factors for high Ki-67 risk stratification. The area under the curve (AUC) of the clinical model was 0.77, while those of the radiomic and DTL models were 0.81 and 0.87, respectively, for the prediction of high Ki-67 risk stratification, and the nomogram model achieved a better AUC of 0.92. The median RFS times for patients with high and low Ki-67 risk stratification were 33.00 months and 66.73 months, respectively (P < 0.001). Additionally, patients who were predicted to have high Ki-67 risk stratification by the nomogram model had a lower median RFS than those who were predicted to have low Ki-67 risk stratification (33.53 vs 66.74 months, P = 0.007).
Conclusion: Our developed nomogram model demonstrated good performance in predicting Ki-67 risk stratification and predicting survival outcomes in patients with HCC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


