{"title":"膈超声预测心脏手术后急性呼吸窘迫综合征患者脱机成功率:中国的一项前瞻性观察研究","authors":"Yuan-Qin Huang, Pei Yu, Dou-Dou Xiang, Quan Gan","doi":"10.4266/acc.004320","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To explore the value of the diaphragm thickness fraction (TF) and diaphragm mobility (DM) measured by ultrasound for predicting ventilator withdrawal success in patients with acute respiratory distress syndrome (ARDS) after cardiac surgery.</p><p><strong>Methods: </strong>This study included 246 patients undergoing the spontaneous breathing trial. Diaphragmatic function was evaluated by ultrasound, including the diaphragm thickness at the end of calm breathing (thickness of the diaphragm at functional residual capacity [TdiFRC]) and the maximum diaphragm thickness at the end of inspiration (thickness of the diaphragm at full vital capacity [TdiFVC]); TF=(TdiFVC-TdiFRC)/TdiFRC×100%. DM, the oxygenation index (the ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen), and the rapid shallow breathing index (RSBI) were measured.</p><p><strong>Results: </strong>Successful liberation from mechanical ventilation was observed in 209 patients. There were no significant differences in the TdiFRC (0.3±0.1 cm vs. 0.3±0.1 cm) or TdiFVC (0.3±0.1 cm vs. 0.2±0.1 cm) between the ventilator withdrawal success group and the ventilator withdrawal failure group (P>0.05). The TF was greater in the ventilator withdrawal success group than in the ventilator withdrawal failure group (40.8%±15.8% vs. 37.7%±9.2%, P<0.01). DM in the ventilator withdrawal success group was greater than that in the ventilator withdrawal failure group (1.5±0.5 cm vs. 1.2±0.4 cm, P=0.040). The RSBI was lower in the ventilator withdrawal success group than in the ventilator withdrawal failure group (74.3±25.6 breaths·min-1·L -1 vs. 89.9±34.5 breaths·min-1·L -1, P<0.01).</p><p><strong>Conclusions: </strong>Diaphragmatic ultrasound can be used to predict the success of ventilator withdrawal in patients with ARDS.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":"40 3","pages":"435-443"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12408480/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diaphragm ultrasound for predicting weaning success in post-cardiac surgery acute respiratory distress syndrome patients: a prospective observational study in China.\",\"authors\":\"Yuan-Qin Huang, Pei Yu, Dou-Dou Xiang, Quan Gan\",\"doi\":\"10.4266/acc.004320\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>To explore the value of the diaphragm thickness fraction (TF) and diaphragm mobility (DM) measured by ultrasound for predicting ventilator withdrawal success in patients with acute respiratory distress syndrome (ARDS) after cardiac surgery.</p><p><strong>Methods: </strong>This study included 246 patients undergoing the spontaneous breathing trial. Diaphragmatic function was evaluated by ultrasound, including the diaphragm thickness at the end of calm breathing (thickness of the diaphragm at functional residual capacity [TdiFRC]) and the maximum diaphragm thickness at the end of inspiration (thickness of the diaphragm at full vital capacity [TdiFVC]); TF=(TdiFVC-TdiFRC)/TdiFRC×100%. DM, the oxygenation index (the ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen), and the rapid shallow breathing index (RSBI) were measured.</p><p><strong>Results: </strong>Successful liberation from mechanical ventilation was observed in 209 patients. There were no significant differences in the TdiFRC (0.3±0.1 cm vs. 0.3±0.1 cm) or TdiFVC (0.3±0.1 cm vs. 0.2±0.1 cm) between the ventilator withdrawal success group and the ventilator withdrawal failure group (P>0.05). The TF was greater in the ventilator withdrawal success group than in the ventilator withdrawal failure group (40.8%±15.8% vs. 37.7%±9.2%, P<0.01). DM in the ventilator withdrawal success group was greater than that in the ventilator withdrawal failure group (1.5±0.5 cm vs. 1.2±0.4 cm, P=0.040). The RSBI was lower in the ventilator withdrawal success group than in the ventilator withdrawal failure group (74.3±25.6 breaths·min-1·L -1 vs. 89.9±34.5 breaths·min-1·L -1, P<0.01).</p><p><strong>Conclusions: </strong>Diaphragmatic ultrasound can be used to predict the success of ventilator withdrawal in patients with ARDS.</p>\",\"PeriodicalId\":44118,\"journal\":{\"name\":\"Acute and Critical Care\",\"volume\":\"40 3\",\"pages\":\"435-443\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12408480/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acute and Critical Care\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4266/acc.004320\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.004320","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:探讨超声测量膈膜厚度分数(TF)和膈膜活度(DM)对心脏手术后急性呼吸窘迫综合征(ARDS)患者脱机成功率的预测价值。方法:本研究纳入246例患者进行自主呼吸试验。超声评估膈肌功能,包括平静呼吸结束时的膈肌厚度(功能剩余容量时的膈肌厚度[TdiFRC])和吸气结束时的最大膈肌厚度(全肺活量时的膈肌厚度[TdiFVC]);TF = (TdiFVC-TdiFRC) / TdiFRC×100%。测定DM、氧合指数(动脉氧分压与吸入氧分数之比)和快速浅呼吸指数(RSBI)。结果:209例患者成功脱离机械通气。TdiFRC(0.3±0.1 cm vs. 0.3±0.1 cm)和TdiFVC(0.3±0.1 cm vs. 0.2±0.1 cm)在呼吸机退出成功组和呼吸机退出失败组之间无显著差异(P < 0.05)。呼吸机撤机成功组的TF高于呼吸机撤机失败组(40.8%±15.8% vs. 37.7%±9.2%)。结论:膈超声可用于预测ARDS患者的呼吸机撤机成功率。
Diaphragm ultrasound for predicting weaning success in post-cardiac surgery acute respiratory distress syndrome patients: a prospective observational study in China.
Background: To explore the value of the diaphragm thickness fraction (TF) and diaphragm mobility (DM) measured by ultrasound for predicting ventilator withdrawal success in patients with acute respiratory distress syndrome (ARDS) after cardiac surgery.
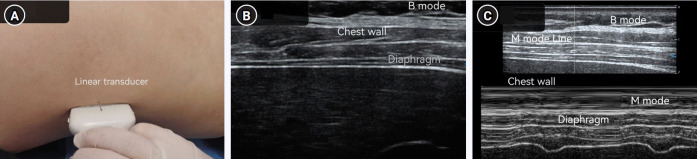
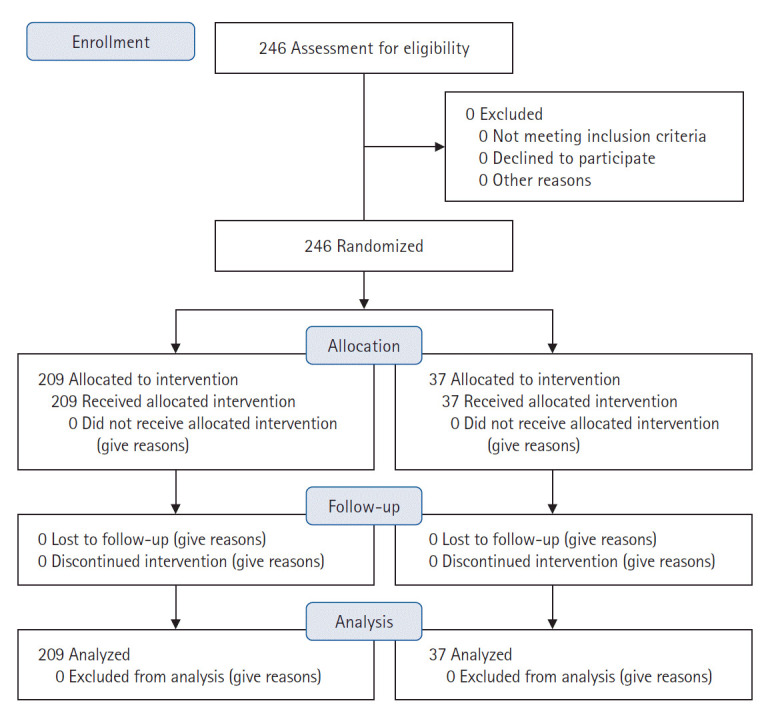
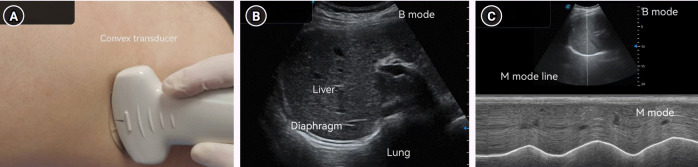
Methods: This study included 246 patients undergoing the spontaneous breathing trial. Diaphragmatic function was evaluated by ultrasound, including the diaphragm thickness at the end of calm breathing (thickness of the diaphragm at functional residual capacity [TdiFRC]) and the maximum diaphragm thickness at the end of inspiration (thickness of the diaphragm at full vital capacity [TdiFVC]); TF=(TdiFVC-TdiFRC)/TdiFRC×100%. DM, the oxygenation index (the ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen), and the rapid shallow breathing index (RSBI) were measured.
Results: Successful liberation from mechanical ventilation was observed in 209 patients. There were no significant differences in the TdiFRC (0.3±0.1 cm vs. 0.3±0.1 cm) or TdiFVC (0.3±0.1 cm vs. 0.2±0.1 cm) between the ventilator withdrawal success group and the ventilator withdrawal failure group (P>0.05). The TF was greater in the ventilator withdrawal success group than in the ventilator withdrawal failure group (40.8%±15.8% vs. 37.7%±9.2%, P<0.01). DM in the ventilator withdrawal success group was greater than that in the ventilator withdrawal failure group (1.5±0.5 cm vs. 1.2±0.4 cm, P=0.040). The RSBI was lower in the ventilator withdrawal success group than in the ventilator withdrawal failure group (74.3±25.6 breaths·min-1·L -1 vs. 89.9±34.5 breaths·min-1·L -1, P<0.01).
Conclusions: Diaphragmatic ultrasound can be used to predict the success of ventilator withdrawal in patients with ARDS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


