Rachel B Issaka, Laura Matrajt, Pedro Nascimento de Lima, Carolyn M Rutter
{"title":"促进结肠镜检查完成的拼车计划的成本效益模型。","authors":"Rachel B Issaka, Laura Matrajt, Pedro Nascimento de Lima, Carolyn M Rutter","doi":"10.1001/jamanetworkopen.2025.30515","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>In colorectal cancer (CRC) screening, too many patients fail to receive follow-up colonoscopy after an abnormal fecal immunochemical test (FIT), and transportation is a frequently reported barrier.</p><p><strong>Objective: </strong>To determine the outcomes and cost-effectiveness of providing a rideshare intervention to patients with abnormal FIT results.</p><p><strong>Design, setting, and participants: </strong>The CRC-Simulated Population Model for Incidence and Natural History microsimulation model was used to simulate the outcomes and cost-effectiveness of a rideshare intervention to improve colonoscopy completion in a population-based CRC screening program. Cohorts were adherent to annual FIT-based screening; baseline analyses assumed that 35% would complete a follow-up colonoscopy. Data were analyzed from November 14, 2023, to July 8, 2025.</p><p><strong>Intervention: </strong>A $40 or $100 rideshare to increase completion of follow-up colonoscopy.</p><p><strong>Main outcomes and measures: </strong>Lifetime outcomes included the number of CRC cases, deaths, and life-years gained (LYG) per 1000 people screened and costs associated with improved completion of a colonoscopy after an abnormal FIT result.</p><p><strong>Results: </strong>Four single-age cohorts (ages 45, 55, 65, and 70 years on January 1, 2024) of 10 million people each were simulated. In cohorts with similar sex distribution as the US population (aged 45 years, 50.0% male; aged 55 years, 49.4% male); aged 65 years, 48.0% male; and aged 70 years, 46.9% male), compared with no intervention, using a rideshare intervention starting at age 45 years that costs $100 per ride to increase colonoscopy completion from 35% to 70% was associated with a reduction in CRC cases per 1000 by 26.3% (30.7 vs 41.6 cases per 1000), CRC deaths per 1000 by 32.5% (9.8 vs 14.6 cases per 1000), 24.9 LYG per 1000, and at $100 per ride cost $43 308 per 1000 people screened and saved $330 587 per 1000 people screened.</p><p><strong>Conclusions and relevance: </strong>In a microsimulation model, increasing colonoscopy completion in a population with abnormal FIT results via a rideshare intervention was cost saving up to $100 per ride due to the combined outcome of cancer prevention and early detection.</p>","PeriodicalId":14694,"journal":{"name":"JAMA Network Open","volume":"8 9","pages":"e2530515"},"PeriodicalIF":9.7000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12411970/pdf/","citationCount":"0","resultStr":"{\"title\":\"Modeled Cost-Effectiveness of a Rideshare Program to Facilitate Colonoscopy Completion.\",\"authors\":\"Rachel B Issaka, Laura Matrajt, Pedro Nascimento de Lima, Carolyn M Rutter\",\"doi\":\"10.1001/jamanetworkopen.2025.30515\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>In colorectal cancer (CRC) screening, too many patients fail to receive follow-up colonoscopy after an abnormal fecal immunochemical test (FIT), and transportation is a frequently reported barrier.</p><p><strong>Objective: </strong>To determine the outcomes and cost-effectiveness of providing a rideshare intervention to patients with abnormal FIT results.</p><p><strong>Design, setting, and participants: </strong>The CRC-Simulated Population Model for Incidence and Natural History microsimulation model was used to simulate the outcomes and cost-effectiveness of a rideshare intervention to improve colonoscopy completion in a population-based CRC screening program. Cohorts were adherent to annual FIT-based screening; baseline analyses assumed that 35% would complete a follow-up colonoscopy. Data were analyzed from November 14, 2023, to July 8, 2025.</p><p><strong>Intervention: </strong>A $40 or $100 rideshare to increase completion of follow-up colonoscopy.</p><p><strong>Main outcomes and measures: </strong>Lifetime outcomes included the number of CRC cases, deaths, and life-years gained (LYG) per 1000 people screened and costs associated with improved completion of a colonoscopy after an abnormal FIT result.</p><p><strong>Results: </strong>Four single-age cohorts (ages 45, 55, 65, and 70 years on January 1, 2024) of 10 million people each were simulated. In cohorts with similar sex distribution as the US population (aged 45 years, 50.0% male; aged 55 years, 49.4% male); aged 65 years, 48.0% male; and aged 70 years, 46.9% male), compared with no intervention, using a rideshare intervention starting at age 45 years that costs $100 per ride to increase colonoscopy completion from 35% to 70% was associated with a reduction in CRC cases per 1000 by 26.3% (30.7 vs 41.6 cases per 1000), CRC deaths per 1000 by 32.5% (9.8 vs 14.6 cases per 1000), 24.9 LYG per 1000, and at $100 per ride cost $43 308 per 1000 people screened and saved $330 587 per 1000 people screened.</p><p><strong>Conclusions and relevance: </strong>In a microsimulation model, increasing colonoscopy completion in a population with abnormal FIT results via a rideshare intervention was cost saving up to $100 per ride due to the combined outcome of cancer prevention and early detection.</p>\",\"PeriodicalId\":14694,\"journal\":{\"name\":\"JAMA Network Open\",\"volume\":\"8 9\",\"pages\":\"e2530515\"},\"PeriodicalIF\":9.7000,\"publicationDate\":\"2025-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12411970/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Network Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1001/jamanetworkopen.2025.30515\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Network Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamanetworkopen.2025.30515","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
重要性:在结直肠癌(CRC)筛查中,太多患者在粪便免疫化学试验(FIT)异常后未能接受随访结肠镜检查,而运输是经常报道的障碍。目的:确定为FIT结果异常的患者提供拼车干预的结果和成本效益。设计、设置和参与者:使用CRC模拟人群发病率模型和自然历史微观模拟模型来模拟拼车干预的结果和成本效益,以提高基于人群的CRC筛查项目的结肠镜检查完成度。队列坚持每年进行基于fit的筛查;基线分析假设35%的患者会完成后续结肠镜检查。数据分析时间为2023年11月14日至2025年7月8日。干预措施:40美元或100美元的拼车,以提高后续结肠镜检查的完成度。主要结局和指标:终生结局包括CRC病例数、死亡和每1000名筛查者获得的生命年(LYG),以及在FIT结果异常后结肠镜检查完成程度提高的相关费用。结果:模拟了四个单年龄队列(2024年1月1日的年龄分别为45岁、55岁、65岁和70岁),每个队列有1000万人。在与美国人口性别分布相似的队列中(45岁,50.0%男性;55岁,49.4%男性);65岁,男性48.0%;和70岁,46.9%为男性),而没有干预,从45岁开始使用rideshare干预成本100美元每骑结肠镜检查完成从35%提高到70%,减少在CRC情况下每1000 26.3% (30.7 vs 41.6情况下每1000人),CRC死亡每1000 32.5% (9.8 vs 14.6情况下每1000人),每1000人24.9来讲,每骑43 308美元100美元每1000人筛选并保存每1000人587 330美元 筛选。结论和相关性:在微观模拟模型中,由于癌症预防和早期发现的综合结果,通过拼车干预,在FIT结果异常的人群中增加结肠镜检查的完成度,每次乘坐可节省高达100美元的成本。
Modeled Cost-Effectiveness of a Rideshare Program to Facilitate Colonoscopy Completion.
Importance: In colorectal cancer (CRC) screening, too many patients fail to receive follow-up colonoscopy after an abnormal fecal immunochemical test (FIT), and transportation is a frequently reported barrier.
Objective: To determine the outcomes and cost-effectiveness of providing a rideshare intervention to patients with abnormal FIT results.
Design, setting, and participants: The CRC-Simulated Population Model for Incidence and Natural History microsimulation model was used to simulate the outcomes and cost-effectiveness of a rideshare intervention to improve colonoscopy completion in a population-based CRC screening program. Cohorts were adherent to annual FIT-based screening; baseline analyses assumed that 35% would complete a follow-up colonoscopy. Data were analyzed from November 14, 2023, to July 8, 2025.
Intervention: A $40 or $100 rideshare to increase completion of follow-up colonoscopy.
Main outcomes and measures: Lifetime outcomes included the number of CRC cases, deaths, and life-years gained (LYG) per 1000 people screened and costs associated with improved completion of a colonoscopy after an abnormal FIT result.
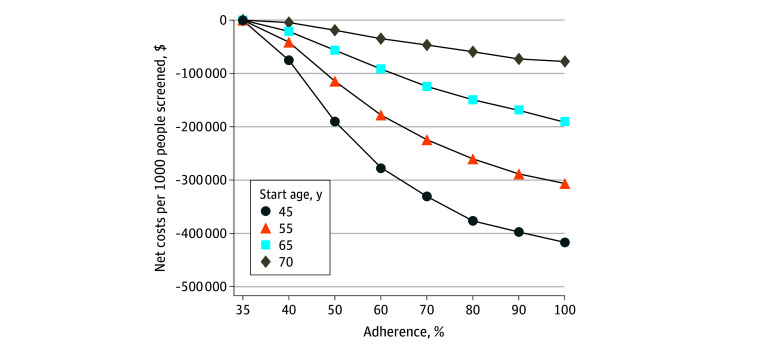
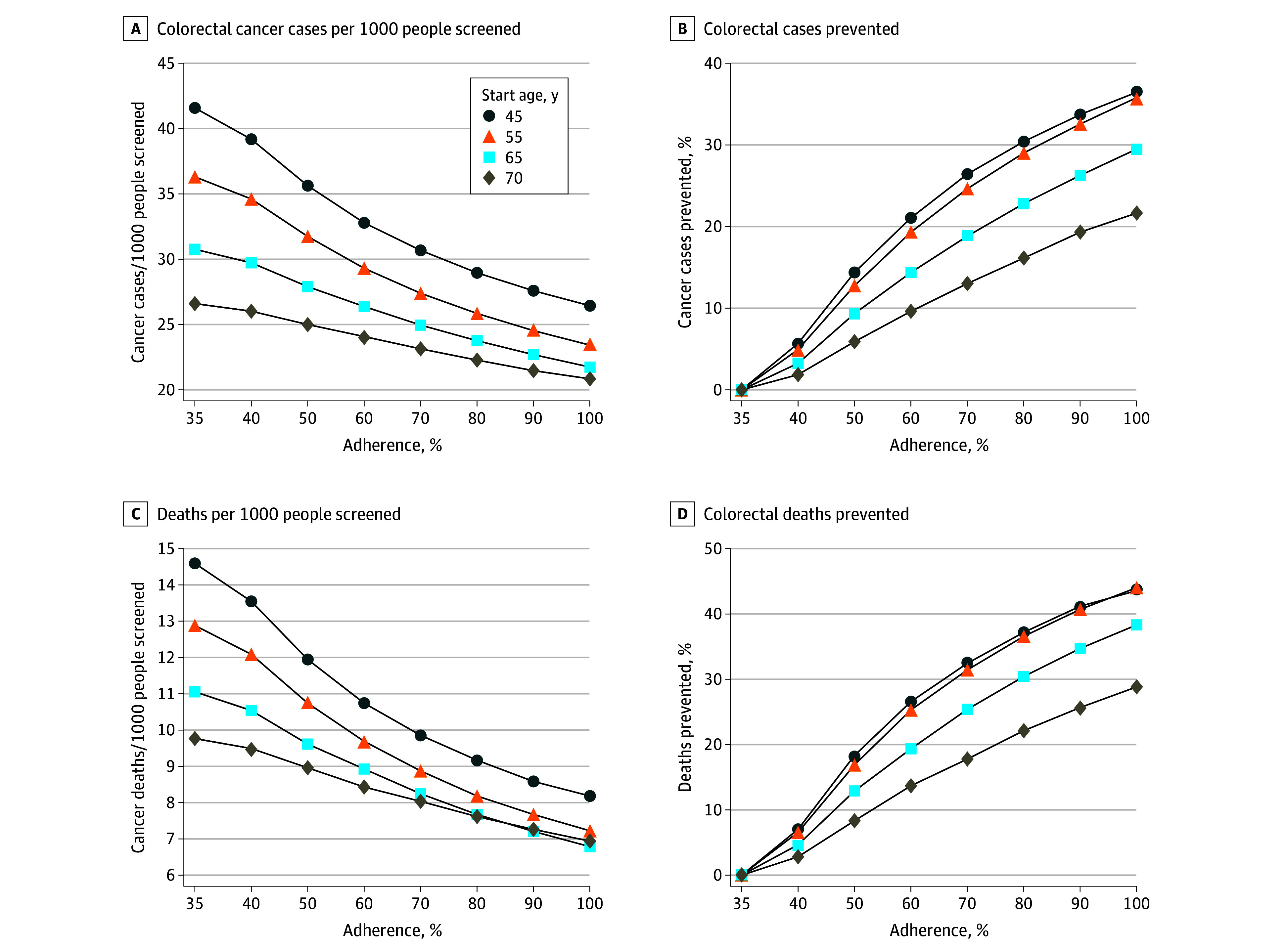
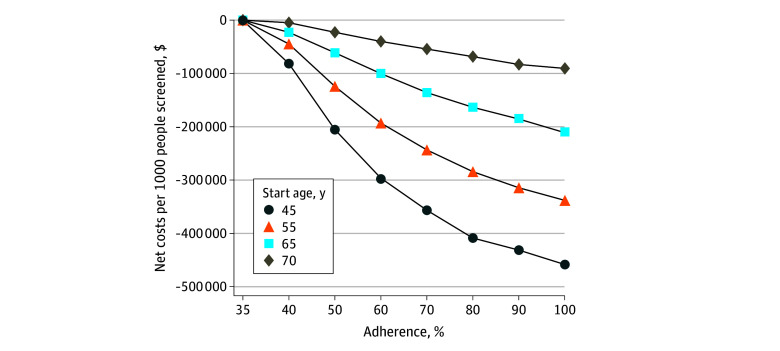
Results: Four single-age cohorts (ages 45, 55, 65, and 70 years on January 1, 2024) of 10 million people each were simulated. In cohorts with similar sex distribution as the US population (aged 45 years, 50.0% male; aged 55 years, 49.4% male); aged 65 years, 48.0% male; and aged 70 years, 46.9% male), compared with no intervention, using a rideshare intervention starting at age 45 years that costs $100 per ride to increase colonoscopy completion from 35% to 70% was associated with a reduction in CRC cases per 1000 by 26.3% (30.7 vs 41.6 cases per 1000), CRC deaths per 1000 by 32.5% (9.8 vs 14.6 cases per 1000), 24.9 LYG per 1000, and at $100 per ride cost $43 308 per 1000 people screened and saved $330 587 per 1000 people screened.
Conclusions and relevance: In a microsimulation model, increasing colonoscopy completion in a population with abnormal FIT results via a rideshare intervention was cost saving up to $100 per ride due to the combined outcome of cancer prevention and early detection.
期刊介绍:
JAMA Network Open, a member of the esteemed JAMA Network, stands as an international, peer-reviewed, open-access general medical journal.The publication is dedicated to disseminating research across various health disciplines and countries, encompassing clinical care, innovation in health care, health policy, and global health.
JAMA Network Open caters to clinicians, investigators, and policymakers, providing a platform for valuable insights and advancements in the medical field. As part of the JAMA Network, a consortium of peer-reviewed general medical and specialty publications, JAMA Network Open contributes to the collective knowledge and understanding within the medical community.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


