Tron Anders Moger, Jon Helgheim Holte, Olav Amundsen, Silje Bjørnsen Haavaag, Øystein Døhl, Line Kildal Bragstad, Ragnhild Hellesø, Trond Tjerbo, Nina Køpke Vøllestad
{"title":"挪威COPD患者短期住院相关的预测因素、医疗保健利用和成本:一项基于登记的分析","authors":"Tron Anders Moger, Jon Helgheim Holte, Olav Amundsen, Silje Bjørnsen Haavaag, Øystein Døhl, Line Kildal Bragstad, Ragnhild Hellesø, Trond Tjerbo, Nina Køpke Vøllestad","doi":"10.2147/CLEP.S521958","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic obstructive pulmonary disease (COPD) incurs significant healthcare costs, often accompanied by multimorbidity. Advanced patients may need short-term stays for rehabilitation, treatment, or respite to maintain home living.</p><p><strong>Aim: </strong>To identify predictors for a first short-term stay and study the healthcare utilization and costs compared with similar patients without a short-term stay.</p><p><strong>Patients and methods: </strong>Data on COPD patients in the cities Oslo and Trondheim 2010-2019 and including information on specialist, primary and long-term care, diagnoses, sociodemographics and -economics were collected from national and municipal registries, resulting in a sample of 24,613 patients. Using discrete time survival models, we identified predictors for a short-term stay. We described the costs before and after admission, and the duration of living at home, compared to non-recipients matched on age, comorbidities and healthcare use.</p><p><strong>Results: </strong>Depression, anxiety, mental disorders, alcoholism, prior hospitalization and reception of home care were associated with higher odds of short-term stays. One to two GP visits for respiratory diseases, being in the top quartile for GP visits for non-respiratory diseases, visits to specialists, and physiotherapist visits for non-respiratory issues were significantly associated with lower odds of short-term institutional stay. Patients admitted to short-term stays incurred markedly higher costs both in the year before admission and during subsequent years compared to matched non-recipients, primarily due to increased use of inpatient and home care services.</p><p><strong>Conclusion: </strong>Prior receipt of home care, unlike standard outpatient services, was linked to a higher likelihood of short-term stays. This suggests that some outpatient services may delay the need for such stays, or that patients already in municipal services are more readily admitted. Additionally, patients with psychosocial issues may have greater care needs, indicating that resource allocation aligns with these needs. The findings suggest that by the time short-term stays are required, health deterioration has already become considerable.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":"17 ","pages":"707-719"},"PeriodicalIF":3.2000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399859/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictors, Healthcare Utilization and Costs Related to Short-Term Stays in Patients with COPD: A Registry-Based Analysis in Norway.\",\"authors\":\"Tron Anders Moger, Jon Helgheim Holte, Olav Amundsen, Silje Bjørnsen Haavaag, Øystein Døhl, Line Kildal Bragstad, Ragnhild Hellesø, Trond Tjerbo, Nina Køpke Vøllestad\",\"doi\":\"10.2147/CLEP.S521958\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chronic obstructive pulmonary disease (COPD) incurs significant healthcare costs, often accompanied by multimorbidity. Advanced patients may need short-term stays for rehabilitation, treatment, or respite to maintain home living.</p><p><strong>Aim: </strong>To identify predictors for a first short-term stay and study the healthcare utilization and costs compared with similar patients without a short-term stay.</p><p><strong>Patients and methods: </strong>Data on COPD patients in the cities Oslo and Trondheim 2010-2019 and including information on specialist, primary and long-term care, diagnoses, sociodemographics and -economics were collected from national and municipal registries, resulting in a sample of 24,613 patients. Using discrete time survival models, we identified predictors for a short-term stay. We described the costs before and after admission, and the duration of living at home, compared to non-recipients matched on age, comorbidities and healthcare use.</p><p><strong>Results: </strong>Depression, anxiety, mental disorders, alcoholism, prior hospitalization and reception of home care were associated with higher odds of short-term stays. One to two GP visits for respiratory diseases, being in the top quartile for GP visits for non-respiratory diseases, visits to specialists, and physiotherapist visits for non-respiratory issues were significantly associated with lower odds of short-term institutional stay. Patients admitted to short-term stays incurred markedly higher costs both in the year before admission and during subsequent years compared to matched non-recipients, primarily due to increased use of inpatient and home care services.</p><p><strong>Conclusion: </strong>Prior receipt of home care, unlike standard outpatient services, was linked to a higher likelihood of short-term stays. This suggests that some outpatient services may delay the need for such stays, or that patients already in municipal services are more readily admitted. Additionally, patients with psychosocial issues may have greater care needs, indicating that resource allocation aligns with these needs. The findings suggest that by the time short-term stays are required, health deterioration has already become considerable.</p>\",\"PeriodicalId\":10362,\"journal\":{\"name\":\"Clinical Epidemiology\",\"volume\":\"17 \",\"pages\":\"707-719\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-08-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399859/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/CLEP.S521958\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S521958","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Predictors, Healthcare Utilization and Costs Related to Short-Term Stays in Patients with COPD: A Registry-Based Analysis in Norway.
Background: Chronic obstructive pulmonary disease (COPD) incurs significant healthcare costs, often accompanied by multimorbidity. Advanced patients may need short-term stays for rehabilitation, treatment, or respite to maintain home living.
Aim: To identify predictors for a first short-term stay and study the healthcare utilization and costs compared with similar patients without a short-term stay.
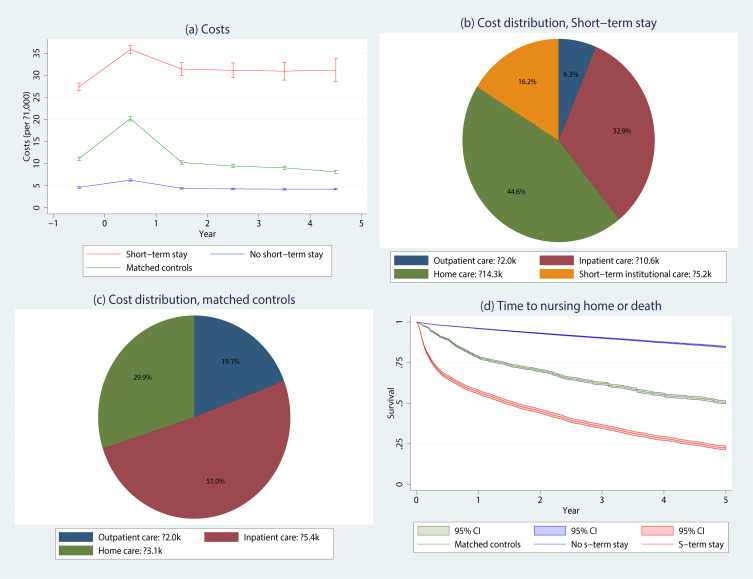
Patients and methods: Data on COPD patients in the cities Oslo and Trondheim 2010-2019 and including information on specialist, primary and long-term care, diagnoses, sociodemographics and -economics were collected from national and municipal registries, resulting in a sample of 24,613 patients. Using discrete time survival models, we identified predictors for a short-term stay. We described the costs before and after admission, and the duration of living at home, compared to non-recipients matched on age, comorbidities and healthcare use.
Results: Depression, anxiety, mental disorders, alcoholism, prior hospitalization and reception of home care were associated with higher odds of short-term stays. One to two GP visits for respiratory diseases, being in the top quartile for GP visits for non-respiratory diseases, visits to specialists, and physiotherapist visits for non-respiratory issues were significantly associated with lower odds of short-term institutional stay. Patients admitted to short-term stays incurred markedly higher costs both in the year before admission and during subsequent years compared to matched non-recipients, primarily due to increased use of inpatient and home care services.
Conclusion: Prior receipt of home care, unlike standard outpatient services, was linked to a higher likelihood of short-term stays. This suggests that some outpatient services may delay the need for such stays, or that patients already in municipal services are more readily admitted. Additionally, patients with psychosocial issues may have greater care needs, indicating that resource allocation aligns with these needs. The findings suggest that by the time short-term stays are required, health deterioration has already become considerable.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


