{"title":"非st段抬高型心肌梗死患者颈前路椎间盘切除术后食管穿孔和融合硬体失败的延迟表现:一个说说性技术说明。","authors":"Tyler Nicole Lackland, Mayur Patel, Kathleen Suzann Botterbush, Joseph J Platz, Mauricio J Avila","doi":"10.25259/SNI_242_2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A 69-year-old male, who underwent a C5-T1 ACDF 5-years prior to arrival, presented with a ventral pharyngeal abscess and esophageal perforation warranting major gastro-esophageal surgery and instrumentation removal.</p><p><strong>Methods: </strong>The case of a patient who underwent a C5-T1 ACDF five years ago was reviewed. A review of past reports of cases of patients who experienced esophageal erosion or perforation following ACDF was conducted.</p><p><strong>Results: </strong>At the age of 69, the patient acutely developed disorientation/agitation and urinary/fecal incontinence. Lab studies showed leukocytosis, an elevated creatine phosphokinase (CPK), and lactic acidosis, while the EKG confirmed a non-ST-elevation myocardial infarction (NSTEMI) with increased troponins. An esophagram revealed esophageal perforation, and a prevertebral C5-C6 abscess, and neck/thoracic CT studies documented 8-9 mm anterior displacement of the right inferior C7 screw with extravasation extending inferiorly into the mediastinum. Surgery consisted of an esophagogastroduodenoscopy, gastric/jejunal tube placement, left neck exploration, and dissection of the esophagus off the anterior instrumentation that was subsequently removed. Despite emergent surgical intervention, the patient expired 5 days postoperatively.</p><p><strong>Conclusion: </strong>Neurosurgical follow-up is warranted in ACDF patients who newly present with findings indicative of with anterior retropharyngeal abscess or esophageal perforation.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"16 ","pages":"299"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361707/pdf/","citationCount":"0","resultStr":"{\"title\":\"Delayed presentation of esophageal perforation from anterior cervical discectomy and fusion hardware failure in a patient presenting with non-ST-elevation myocardial infarction: An illustrative technical note.\",\"authors\":\"Tyler Nicole Lackland, Mayur Patel, Kathleen Suzann Botterbush, Joseph J Platz, Mauricio J Avila\",\"doi\":\"10.25259/SNI_242_2025\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A 69-year-old male, who underwent a C5-T1 ACDF 5-years prior to arrival, presented with a ventral pharyngeal abscess and esophageal perforation warranting major gastro-esophageal surgery and instrumentation removal.</p><p><strong>Methods: </strong>The case of a patient who underwent a C5-T1 ACDF five years ago was reviewed. A review of past reports of cases of patients who experienced esophageal erosion or perforation following ACDF was conducted.</p><p><strong>Results: </strong>At the age of 69, the patient acutely developed disorientation/agitation and urinary/fecal incontinence. Lab studies showed leukocytosis, an elevated creatine phosphokinase (CPK), and lactic acidosis, while the EKG confirmed a non-ST-elevation myocardial infarction (NSTEMI) with increased troponins. An esophagram revealed esophageal perforation, and a prevertebral C5-C6 abscess, and neck/thoracic CT studies documented 8-9 mm anterior displacement of the right inferior C7 screw with extravasation extending inferiorly into the mediastinum. Surgery consisted of an esophagogastroduodenoscopy, gastric/jejunal tube placement, left neck exploration, and dissection of the esophagus off the anterior instrumentation that was subsequently removed. Despite emergent surgical intervention, the patient expired 5 days postoperatively.</p><p><strong>Conclusion: </strong>Neurosurgical follow-up is warranted in ACDF patients who newly present with findings indicative of with anterior retropharyngeal abscess or esophageal perforation.</p>\",\"PeriodicalId\":94217,\"journal\":{\"name\":\"Surgical neurology international\",\"volume\":\"16 \",\"pages\":\"299\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361707/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical neurology international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.25259/SNI_242_2025\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_242_2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Delayed presentation of esophageal perforation from anterior cervical discectomy and fusion hardware failure in a patient presenting with non-ST-elevation myocardial infarction: An illustrative technical note.
Background: A 69-year-old male, who underwent a C5-T1 ACDF 5-years prior to arrival, presented with a ventral pharyngeal abscess and esophageal perforation warranting major gastro-esophageal surgery and instrumentation removal.
Methods: The case of a patient who underwent a C5-T1 ACDF five years ago was reviewed. A review of past reports of cases of patients who experienced esophageal erosion or perforation following ACDF was conducted.
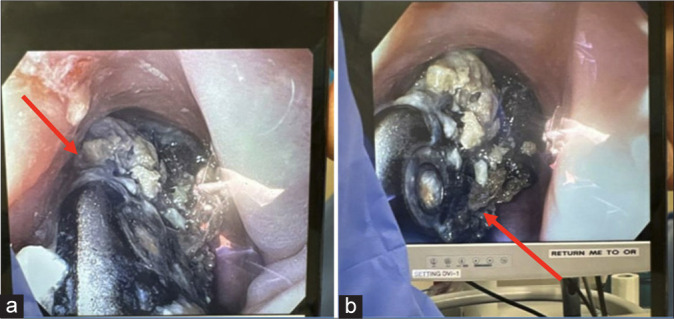
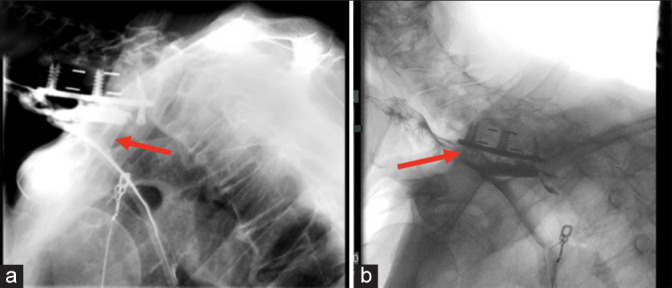
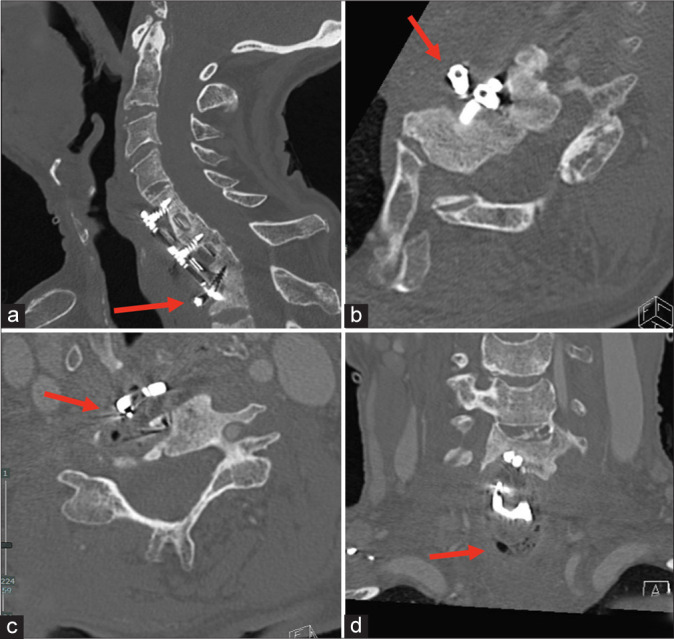
Results: At the age of 69, the patient acutely developed disorientation/agitation and urinary/fecal incontinence. Lab studies showed leukocytosis, an elevated creatine phosphokinase (CPK), and lactic acidosis, while the EKG confirmed a non-ST-elevation myocardial infarction (NSTEMI) with increased troponins. An esophagram revealed esophageal perforation, and a prevertebral C5-C6 abscess, and neck/thoracic CT studies documented 8-9 mm anterior displacement of the right inferior C7 screw with extravasation extending inferiorly into the mediastinum. Surgery consisted of an esophagogastroduodenoscopy, gastric/jejunal tube placement, left neck exploration, and dissection of the esophagus off the anterior instrumentation that was subsequently removed. Despite emergent surgical intervention, the patient expired 5 days postoperatively.
Conclusion: Neurosurgical follow-up is warranted in ACDF patients who newly present with findings indicative of with anterior retropharyngeal abscess or esophageal perforation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


