Alireza Habibi, Michael Anthony Rizzuto, Michael K Tso
{"title":"1例复发性严重头痛患者继发于Chiari 1型畸形的蛛网膜下腔出血:1例报告、影像学和解剖学考虑。","authors":"Alireza Habibi, Michael Anthony Rizzuto, Michael K Tso","doi":"10.25259/SNI_374_2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chiari 1 malformation (CM1) is a structural anomaly characterized by cerebellar tonsillar herniation through the foramen magnum. While typically associated with syringomyelia or hydrocephalus, its potential relationship with subarachnoid hemorrhage (SAH) remains poorly reported in the literature.</p><p><strong>Case description: </strong>We present the case of a 77-year-old woman who experienced recurrent episodes of thunderclap headache, which eventually progressed to altered consciousness following admission. Neuroimaging revealed a SAH involving the fourth ventricle and basal cisterns, alongside cerebellar tonsillar herniation and obstructive hydrocephalus, with no arterial source identified on serial angiography. Magnetic resonance imaging confirmed CM1, with tonsillar descent to the C1 level. The patient underwent suboccipital decompression for refractory intracranial hypertension that prevented weaning from the external ventricular drain. Intraoperative exploration revealed an abnormal posterior spinal vein traversing the arachnoid membrane, which was suspected to be the source of the hemorrhage and was successfully coagulated.</p><p><strong>Conclusion: </strong>To the best of our knowledge, this is the first documented case of CM1 presenting with recurrent SAH in the absence of aneurysmal or arteriovenous pathology. Our findings suggest a possible venous etiology related to anomalous posterior spinal venous drainage, which may have contributed to the hemorrhage and obstructive hydrocephalus. The patient's clinical improvement following Chiari decompression supports the role of surgical intervention in relieving cerebrospinal fluid outflow obstruction and elevated intracranial pressure in such cases. This case highlights the importance of considering venous anomalies in the differential diagnosis of non-aneurysmal SAH and underscores the need for heightened awareness of vascular variations in CM1 patients presenting with acute neurological symptoms.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"16 ","pages":"292"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361651/pdf/","citationCount":"0","resultStr":"{\"title\":\"Subarachnoid hemorrhage secondary to Chiari 1 malformation in a patient presenting with recurrent severe headache: A case report, imaging, and anatomic considerations.\",\"authors\":\"Alireza Habibi, Michael Anthony Rizzuto, Michael K Tso\",\"doi\":\"10.25259/SNI_374_2025\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chiari 1 malformation (CM1) is a structural anomaly characterized by cerebellar tonsillar herniation through the foramen magnum. While typically associated with syringomyelia or hydrocephalus, its potential relationship with subarachnoid hemorrhage (SAH) remains poorly reported in the literature.</p><p><strong>Case description: </strong>We present the case of a 77-year-old woman who experienced recurrent episodes of thunderclap headache, which eventually progressed to altered consciousness following admission. Neuroimaging revealed a SAH involving the fourth ventricle and basal cisterns, alongside cerebellar tonsillar herniation and obstructive hydrocephalus, with no arterial source identified on serial angiography. Magnetic resonance imaging confirmed CM1, with tonsillar descent to the C1 level. The patient underwent suboccipital decompression for refractory intracranial hypertension that prevented weaning from the external ventricular drain. Intraoperative exploration revealed an abnormal posterior spinal vein traversing the arachnoid membrane, which was suspected to be the source of the hemorrhage and was successfully coagulated.</p><p><strong>Conclusion: </strong>To the best of our knowledge, this is the first documented case of CM1 presenting with recurrent SAH in the absence of aneurysmal or arteriovenous pathology. Our findings suggest a possible venous etiology related to anomalous posterior spinal venous drainage, which may have contributed to the hemorrhage and obstructive hydrocephalus. The patient's clinical improvement following Chiari decompression supports the role of surgical intervention in relieving cerebrospinal fluid outflow obstruction and elevated intracranial pressure in such cases. This case highlights the importance of considering venous anomalies in the differential diagnosis of non-aneurysmal SAH and underscores the need for heightened awareness of vascular variations in CM1 patients presenting with acute neurological symptoms.</p>\",\"PeriodicalId\":94217,\"journal\":{\"name\":\"Surgical neurology international\",\"volume\":\"16 \",\"pages\":\"292\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361651/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical neurology international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.25259/SNI_374_2025\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_374_2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Subarachnoid hemorrhage secondary to Chiari 1 malformation in a patient presenting with recurrent severe headache: A case report, imaging, and anatomic considerations.
Background: Chiari 1 malformation (CM1) is a structural anomaly characterized by cerebellar tonsillar herniation through the foramen magnum. While typically associated with syringomyelia or hydrocephalus, its potential relationship with subarachnoid hemorrhage (SAH) remains poorly reported in the literature.
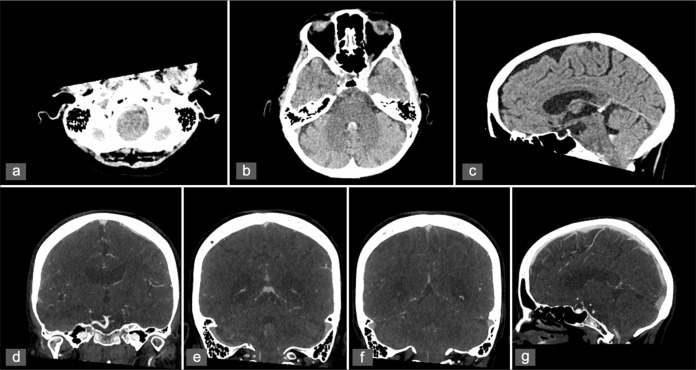
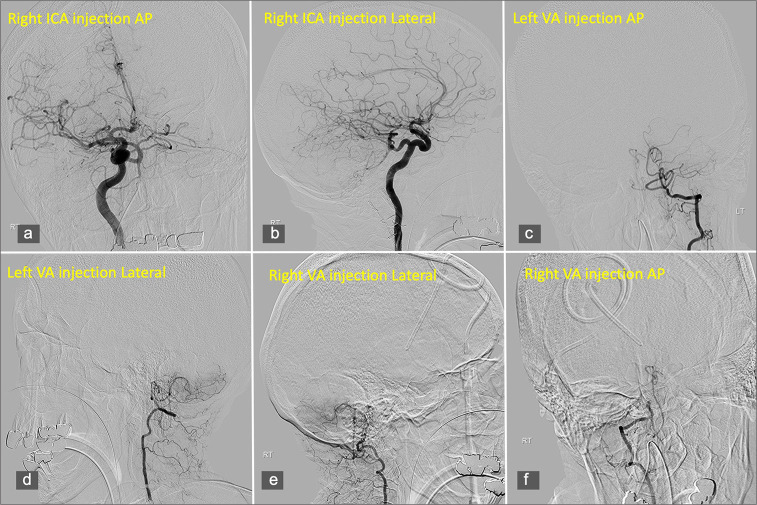
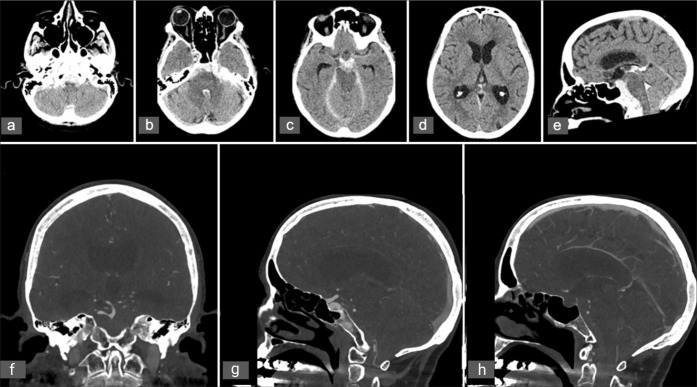
Case description: We present the case of a 77-year-old woman who experienced recurrent episodes of thunderclap headache, which eventually progressed to altered consciousness following admission. Neuroimaging revealed a SAH involving the fourth ventricle and basal cisterns, alongside cerebellar tonsillar herniation and obstructive hydrocephalus, with no arterial source identified on serial angiography. Magnetic resonance imaging confirmed CM1, with tonsillar descent to the C1 level. The patient underwent suboccipital decompression for refractory intracranial hypertension that prevented weaning from the external ventricular drain. Intraoperative exploration revealed an abnormal posterior spinal vein traversing the arachnoid membrane, which was suspected to be the source of the hemorrhage and was successfully coagulated.
Conclusion: To the best of our knowledge, this is the first documented case of CM1 presenting with recurrent SAH in the absence of aneurysmal or arteriovenous pathology. Our findings suggest a possible venous etiology related to anomalous posterior spinal venous drainage, which may have contributed to the hemorrhage and obstructive hydrocephalus. The patient's clinical improvement following Chiari decompression supports the role of surgical intervention in relieving cerebrospinal fluid outflow obstruction and elevated intracranial pressure in such cases. This case highlights the importance of considering venous anomalies in the differential diagnosis of non-aneurysmal SAH and underscores the need for heightened awareness of vascular variations in CM1 patients presenting with acute neurological symptoms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


