{"title":"颈内动脉夹层并舌咽神经功能障碍1例。","authors":"Tomoya Sofue, Megumi Chatani, Hiroyuki Ohnishi","doi":"10.25259/SNI_528_2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Internal carotid artery dissection (ICAD) is an uncommon but important cause of ischemic stroke in young adults, particularly in Asian populations where its incidence is relatively low. While ICAD typically presents with headache, neck pain, or ischemic symptoms, it can also lead to isolated cranial nerve involvement, complicating the diagnostic process.</p><p><strong>Case description: </strong>We report the case of a 45-year-old woman who presented with isolated right-sided glossopharyngeal nerve symptoms - specifically, ageusia and pharyngeal discomfort - along with mild posterior neck pain. Initial evaluation by otolaryngology failed to identify the etiology. Subsequent imaging at our hospital revealed a spontaneous dissection of the right internal carotid artery extending from the third cervical spinal cord level to the proximal petrous segment. Magnetic resonance angiography and digital subtraction angiography confirmed the diagnosis of ICAD. Conservative management with antiplatelet therapy (aspirin 100 mg/day) led to symptom improvement, and follow-up imaging after 180 days demonstrated near-complete resolution of the dissection.</p><p><strong>Conclusion: </strong>This case is noteworthy due to the absence of cerebral ischemic findings and the isolated involvement of the glossopharyngeal nerve, likely due to localized anterolateral expansion of the dissection cavity compressing the pharyngeal branch of the nerve. Although mild styloid process elongation was observed, there was no radiological evidence suggesting Eagle syndrome. This case emphasizes the importance of considering ICAD in the differential diagnosis of lower cranial nerve palsies, even in the absence of stroke or typical neurological signs.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"16 ","pages":"304"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361664/pdf/","citationCount":"0","resultStr":"{\"title\":\"Internal carotid artery dissection presenting with glossopharyngeal nerve dysfunction: A case report.\",\"authors\":\"Tomoya Sofue, Megumi Chatani, Hiroyuki Ohnishi\",\"doi\":\"10.25259/SNI_528_2025\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Internal carotid artery dissection (ICAD) is an uncommon but important cause of ischemic stroke in young adults, particularly in Asian populations where its incidence is relatively low. While ICAD typically presents with headache, neck pain, or ischemic symptoms, it can also lead to isolated cranial nerve involvement, complicating the diagnostic process.</p><p><strong>Case description: </strong>We report the case of a 45-year-old woman who presented with isolated right-sided glossopharyngeal nerve symptoms - specifically, ageusia and pharyngeal discomfort - along with mild posterior neck pain. Initial evaluation by otolaryngology failed to identify the etiology. Subsequent imaging at our hospital revealed a spontaneous dissection of the right internal carotid artery extending from the third cervical spinal cord level to the proximal petrous segment. Magnetic resonance angiography and digital subtraction angiography confirmed the diagnosis of ICAD. Conservative management with antiplatelet therapy (aspirin 100 mg/day) led to symptom improvement, and follow-up imaging after 180 days demonstrated near-complete resolution of the dissection.</p><p><strong>Conclusion: </strong>This case is noteworthy due to the absence of cerebral ischemic findings and the isolated involvement of the glossopharyngeal nerve, likely due to localized anterolateral expansion of the dissection cavity compressing the pharyngeal branch of the nerve. Although mild styloid process elongation was observed, there was no radiological evidence suggesting Eagle syndrome. This case emphasizes the importance of considering ICAD in the differential diagnosis of lower cranial nerve palsies, even in the absence of stroke or typical neurological signs.</p>\",\"PeriodicalId\":94217,\"journal\":{\"name\":\"Surgical neurology international\",\"volume\":\"16 \",\"pages\":\"304\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361664/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical neurology international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.25259/SNI_528_2025\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_528_2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Internal carotid artery dissection presenting with glossopharyngeal nerve dysfunction: A case report.
Background: Internal carotid artery dissection (ICAD) is an uncommon but important cause of ischemic stroke in young adults, particularly in Asian populations where its incidence is relatively low. While ICAD typically presents with headache, neck pain, or ischemic symptoms, it can also lead to isolated cranial nerve involvement, complicating the diagnostic process.
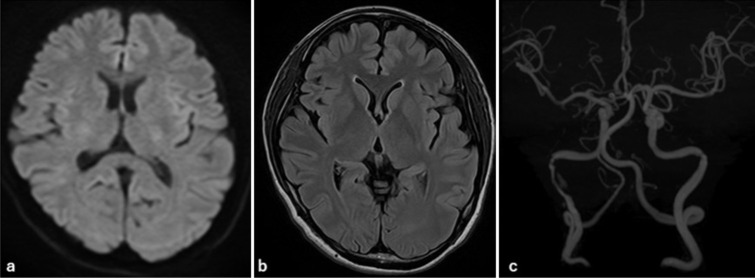
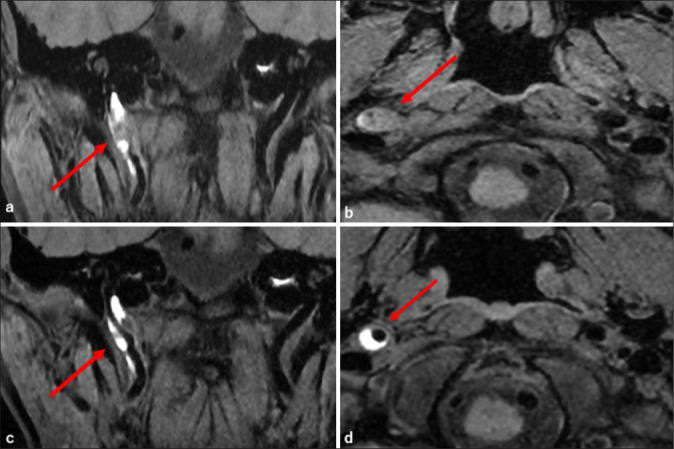
Case description: We report the case of a 45-year-old woman who presented with isolated right-sided glossopharyngeal nerve symptoms - specifically, ageusia and pharyngeal discomfort - along with mild posterior neck pain. Initial evaluation by otolaryngology failed to identify the etiology. Subsequent imaging at our hospital revealed a spontaneous dissection of the right internal carotid artery extending from the third cervical spinal cord level to the proximal petrous segment. Magnetic resonance angiography and digital subtraction angiography confirmed the diagnosis of ICAD. Conservative management with antiplatelet therapy (aspirin 100 mg/day) led to symptom improvement, and follow-up imaging after 180 days demonstrated near-complete resolution of the dissection.
Conclusion: This case is noteworthy due to the absence of cerebral ischemic findings and the isolated involvement of the glossopharyngeal nerve, likely due to localized anterolateral expansion of the dissection cavity compressing the pharyngeal branch of the nerve. Although mild styloid process elongation was observed, there was no radiological evidence suggesting Eagle syndrome. This case emphasizes the importance of considering ICAD in the differential diagnosis of lower cranial nerve palsies, even in the absence of stroke or typical neurological signs.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


