{"title":"围手术期降压药及其对非心脏手术患者功能下降和死亡率的影响。","authors":"Rena Suzukawa, Shintaro Mandai, Yuta Nakano, Shunsuke Inaba, Hisazumi Matsuki, Yutaro Mori, Fumiaki Ando, Takayasu Mori, Koichiro Susa, Soichiro Iimori, Shotaro Naito, Eisei Sohara, Tatemitsu Rai, Kiyohide Fushimi, Shinichi Uchida","doi":"10.1093/ehjopen/oeaf096","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The association between perioperative antihypertensive drugs and mortality as well as physical function in non-cardiac surgeries remains unclear. We aimed to clarify the association between six antihypertensive classes and postoperative outcomes.</p><p><strong>Methods and results: </strong>This observational cohort study involved adults undergoing non-cardiac surgeries between 2014 and 2019 using an administrative claims database. We recruited 408 810 patients who continuously used any class of antihypertensive medication both pre- and postoperatively and 2 190 064 non-continuous users aged ≥50 years who underwent five different types of non-cardiac surgeries. The risk for overall death or functional decline, defined as a ≥20% decrease in the Barthel Index score during hospitalization, was determined using multivariable logistic regression models. All-cause deaths or functional decline occurred in 4228 (1.0%) users and 17 978 (0.8%) non-users or 20 625 (5.0%) users and 66 218 (3.0%) non-users, respectively. Among single-class users, angiotensin-converting enzyme inhibitors (ACEis) or angiotensin II receptor blockers (ARBs) showed a multivariable odds ratio (OR) of 0.74 [95% confidence interval (CI) 0.62-0.89 vs. thiazide/thiazide-like diuretics (TH)] for the composite of mortality and functional decline. Among recipients of two medication classes, calcium receptor blockers (CCBs)/ACEi or ARB usage was associated with the lowest risk for composite outcome (OR, 0.86; 95% CI, 0.81-0.91 vs. TH/CCBs). The combinations of the ≥3 classes, including TH/CCB/ACEi or ARB, displayed the lowest odds for the composite outcome. In orthopaedic surgery and gastrointestinal resection, ACEis or ARBs were associated with better survival and physical function.</p><p><strong>Conclusion: </strong>Perioperative use of ACEis or ARBs is associated with favourable outcomes in non-cardiac surgeries.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 4","pages":"oeaf096"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12393147/pdf/","citationCount":"0","resultStr":"{\"title\":\"Perioperative antihypertensive medications and effects on functional decline and mortality in non-cardiac surgery.\",\"authors\":\"Rena Suzukawa, Shintaro Mandai, Yuta Nakano, Shunsuke Inaba, Hisazumi Matsuki, Yutaro Mori, Fumiaki Ando, Takayasu Mori, Koichiro Susa, Soichiro Iimori, Shotaro Naito, Eisei Sohara, Tatemitsu Rai, Kiyohide Fushimi, Shinichi Uchida\",\"doi\":\"10.1093/ehjopen/oeaf096\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The association between perioperative antihypertensive drugs and mortality as well as physical function in non-cardiac surgeries remains unclear. We aimed to clarify the association between six antihypertensive classes and postoperative outcomes.</p><p><strong>Methods and results: </strong>This observational cohort study involved adults undergoing non-cardiac surgeries between 2014 and 2019 using an administrative claims database. We recruited 408 810 patients who continuously used any class of antihypertensive medication both pre- and postoperatively and 2 190 064 non-continuous users aged ≥50 years who underwent five different types of non-cardiac surgeries. The risk for overall death or functional decline, defined as a ≥20% decrease in the Barthel Index score during hospitalization, was determined using multivariable logistic regression models. All-cause deaths or functional decline occurred in 4228 (1.0%) users and 17 978 (0.8%) non-users or 20 625 (5.0%) users and 66 218 (3.0%) non-users, respectively. Among single-class users, angiotensin-converting enzyme inhibitors (ACEis) or angiotensin II receptor blockers (ARBs) showed a multivariable odds ratio (OR) of 0.74 [95% confidence interval (CI) 0.62-0.89 vs. thiazide/thiazide-like diuretics (TH)] for the composite of mortality and functional decline. Among recipients of two medication classes, calcium receptor blockers (CCBs)/ACEi or ARB usage was associated with the lowest risk for composite outcome (OR, 0.86; 95% CI, 0.81-0.91 vs. TH/CCBs). The combinations of the ≥3 classes, including TH/CCB/ACEi or ARB, displayed the lowest odds for the composite outcome. In orthopaedic surgery and gastrointestinal resection, ACEis or ARBs were associated with better survival and physical function.</p><p><strong>Conclusion: </strong>Perioperative use of ACEis or ARBs is associated with favourable outcomes in non-cardiac surgeries.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 4\",\"pages\":\"oeaf096\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12393147/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf096\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf096","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:围手术期降压药与非心脏手术患者死亡率和身体功能的关系尚不清楚。我们的目的是澄清六种抗高血压药物类别与术后预后之间的关系。方法和结果:这项观察性队列研究涉及2014年至2019年期间接受非心脏手术的成年人,使用行政索赔数据库。我们招募了408810名在术前和术后持续使用任何类别降压药物的患者,以及219064名年龄≥50岁、接受5种不同类型非心脏手术的非连续使用降压药物的患者。总体死亡或功能下降的风险,定义为住院期间Barthel指数评分下降≥20%,采用多变量logistic回归模型确定。全因死亡或功能下降分别发生在4228例(1.0%)使用者和17978例(0.8%)非使用者或20625例(5.0%)使用者和66218例(3.0%)非使用者。在单一类别的使用者中,血管紧张素转换酶抑制剂(ACEis)或血管紧张素II受体阻滞剂(ARBs)在死亡率和功能下降的综合方面的多变量优势比(or)为0.74[95%置信区间(CI) 0.62-0.89 vs.噻嗪类/噻嗪类利尿剂(TH)]。在两种药物类别的接受者中,钙受体阻滞剂(CCBs)/ACEi或ARB的使用与复合结局的最低风险相关(or, 0.86; 95% CI, 0.81-0.91 vs TH/CCBs)。包括TH/CCB/ACEi或ARB在内的≥3个类别的组合显示出最低的综合结局几率。在骨科手术和胃肠道切除术中,ACEis或arb与更好的生存和身体功能相关。结论:在非心脏手术中,围手术期使用acei或arb与良好的预后相关。
Perioperative antihypertensive medications and effects on functional decline and mortality in non-cardiac surgery.
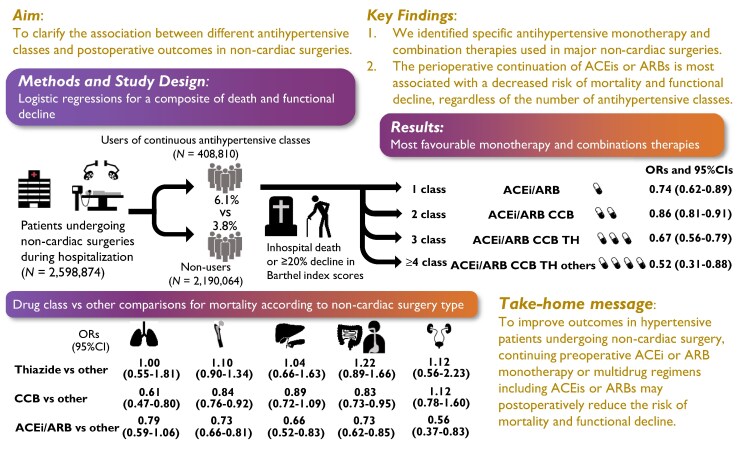
Aims: The association between perioperative antihypertensive drugs and mortality as well as physical function in non-cardiac surgeries remains unclear. We aimed to clarify the association between six antihypertensive classes and postoperative outcomes.
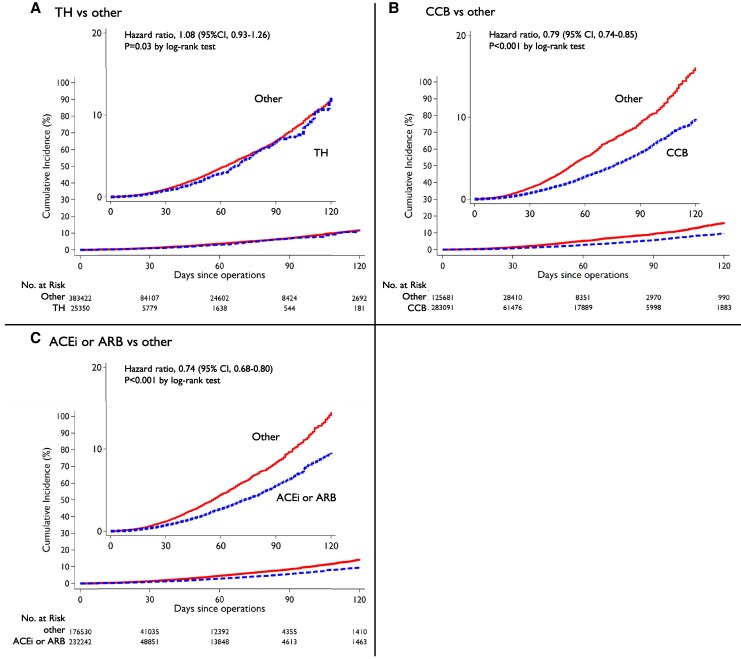
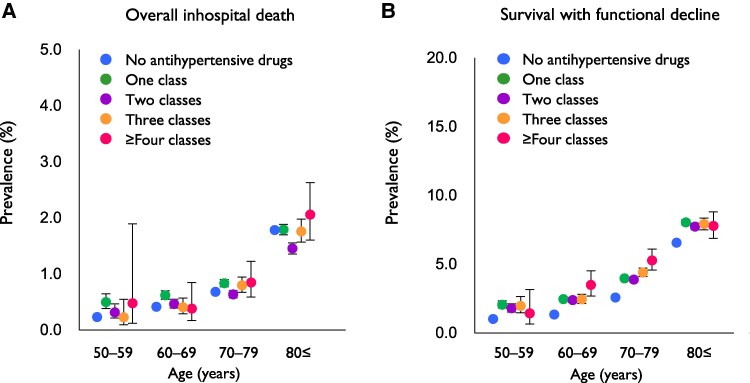
Methods and results: This observational cohort study involved adults undergoing non-cardiac surgeries between 2014 and 2019 using an administrative claims database. We recruited 408 810 patients who continuously used any class of antihypertensive medication both pre- and postoperatively and 2 190 064 non-continuous users aged ≥50 years who underwent five different types of non-cardiac surgeries. The risk for overall death or functional decline, defined as a ≥20% decrease in the Barthel Index score during hospitalization, was determined using multivariable logistic regression models. All-cause deaths or functional decline occurred in 4228 (1.0%) users and 17 978 (0.8%) non-users or 20 625 (5.0%) users and 66 218 (3.0%) non-users, respectively. Among single-class users, angiotensin-converting enzyme inhibitors (ACEis) or angiotensin II receptor blockers (ARBs) showed a multivariable odds ratio (OR) of 0.74 [95% confidence interval (CI) 0.62-0.89 vs. thiazide/thiazide-like diuretics (TH)] for the composite of mortality and functional decline. Among recipients of two medication classes, calcium receptor blockers (CCBs)/ACEi or ARB usage was associated with the lowest risk for composite outcome (OR, 0.86; 95% CI, 0.81-0.91 vs. TH/CCBs). The combinations of the ≥3 classes, including TH/CCB/ACEi or ARB, displayed the lowest odds for the composite outcome. In orthopaedic surgery and gastrointestinal resection, ACEis or ARBs were associated with better survival and physical function.
Conclusion: Perioperative use of ACEis or ARBs is associated with favourable outcomes in non-cardiac surgeries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


