{"title":"经颅多普勒评价开颅术后脑血流动力学。","authors":"Lotfi Rebai, Wissal Nsiri, Firas Kalai, Sabrine Ben Brahem, Olfa Faten, Ichraf Ardhaoui","doi":"10.25259/SNI_423_2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Craniotomy for supratentorial tumor resection can alter cerebral hemodynamics, potentially leading to post-operative complications. Transcranial color-coded duplex sonography (TCCD) provides a noninvasive method for evaluating cerebral perfusion and predicting outcomes. The objective of this study was to assess the prognostic value of TCCD parameters, particularly pulsatility index (PI) and diastolic velocity (DV), in predicting post-operative complications following elective craniotomy for supratentorial tumor resection.</p><p><strong>Methods: </strong>This prospective, observational study included 48 adult patients undergoing supratentorial tumor resection. TCCD was performed preoperatively and postoperatively to measure PI, systolic velocity (SV), DV, and mean velocity (MV). Patients with signs of intracranial pressure hypertension (high) were identified based on clinical and radiological parameters. Post-operative clinical and radiological complications were recorded. ROC curve analyses were performed to determine the predictive value of transcranial Doppler parameters.</p><p><strong>Results: </strong>Post-operative SV and MV significantly increased compared to pre-operative values (<i>P</i> = 0.008 and <i>P</i> = 0.037, respectively), while PI and DV remained stable. Pre-operative elevated PI and decreased DV were significantly associated with post-operative complications, including delayed awakening and ischemia. Postoperative PI predicted ischemia with an area under the curve (AUC) of 0.86 and delayed awakening with an AUC of 0.89. Lower DV values were predictive of seizures, ischemia, and delayed awakening. Elevated PI and reduced DV correlated with longer intensive care unit stays.</p><p><strong>Conclusion: </strong>TCCD is a valuable, non-invasive tool for early identification of patients at risk for post-operative complications following craniotomy for tumor resection. Monitoring PI and DV may guide post-operative management and improve outcomes.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"16 ","pages":"308"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361710/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of post-craniotomy cerebral hemodynamic by transcranial Doppler.\",\"authors\":\"Lotfi Rebai, Wissal Nsiri, Firas Kalai, Sabrine Ben Brahem, Olfa Faten, Ichraf Ardhaoui\",\"doi\":\"10.25259/SNI_423_2025\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Craniotomy for supratentorial tumor resection can alter cerebral hemodynamics, potentially leading to post-operative complications. Transcranial color-coded duplex sonography (TCCD) provides a noninvasive method for evaluating cerebral perfusion and predicting outcomes. The objective of this study was to assess the prognostic value of TCCD parameters, particularly pulsatility index (PI) and diastolic velocity (DV), in predicting post-operative complications following elective craniotomy for supratentorial tumor resection.</p><p><strong>Methods: </strong>This prospective, observational study included 48 adult patients undergoing supratentorial tumor resection. TCCD was performed preoperatively and postoperatively to measure PI, systolic velocity (SV), DV, and mean velocity (MV). Patients with signs of intracranial pressure hypertension (high) were identified based on clinical and radiological parameters. Post-operative clinical and radiological complications were recorded. ROC curve analyses were performed to determine the predictive value of transcranial Doppler parameters.</p><p><strong>Results: </strong>Post-operative SV and MV significantly increased compared to pre-operative values (<i>P</i> = 0.008 and <i>P</i> = 0.037, respectively), while PI and DV remained stable. Pre-operative elevated PI and decreased DV were significantly associated with post-operative complications, including delayed awakening and ischemia. Postoperative PI predicted ischemia with an area under the curve (AUC) of 0.86 and delayed awakening with an AUC of 0.89. Lower DV values were predictive of seizures, ischemia, and delayed awakening. Elevated PI and reduced DV correlated with longer intensive care unit stays.</p><p><strong>Conclusion: </strong>TCCD is a valuable, non-invasive tool for early identification of patients at risk for post-operative complications following craniotomy for tumor resection. Monitoring PI and DV may guide post-operative management and improve outcomes.</p>\",\"PeriodicalId\":94217,\"journal\":{\"name\":\"Surgical neurology international\",\"volume\":\"16 \",\"pages\":\"308\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361710/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical neurology international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.25259/SNI_423_2025\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_423_2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Evaluation of post-craniotomy cerebral hemodynamic by transcranial Doppler.
Background: Craniotomy for supratentorial tumor resection can alter cerebral hemodynamics, potentially leading to post-operative complications. Transcranial color-coded duplex sonography (TCCD) provides a noninvasive method for evaluating cerebral perfusion and predicting outcomes. The objective of this study was to assess the prognostic value of TCCD parameters, particularly pulsatility index (PI) and diastolic velocity (DV), in predicting post-operative complications following elective craniotomy for supratentorial tumor resection.
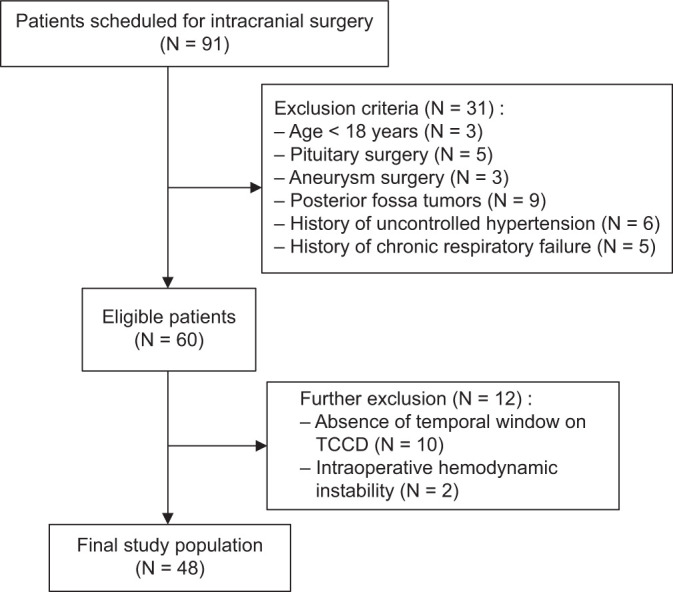
Methods: This prospective, observational study included 48 adult patients undergoing supratentorial tumor resection. TCCD was performed preoperatively and postoperatively to measure PI, systolic velocity (SV), DV, and mean velocity (MV). Patients with signs of intracranial pressure hypertension (high) were identified based on clinical and radiological parameters. Post-operative clinical and radiological complications were recorded. ROC curve analyses were performed to determine the predictive value of transcranial Doppler parameters.
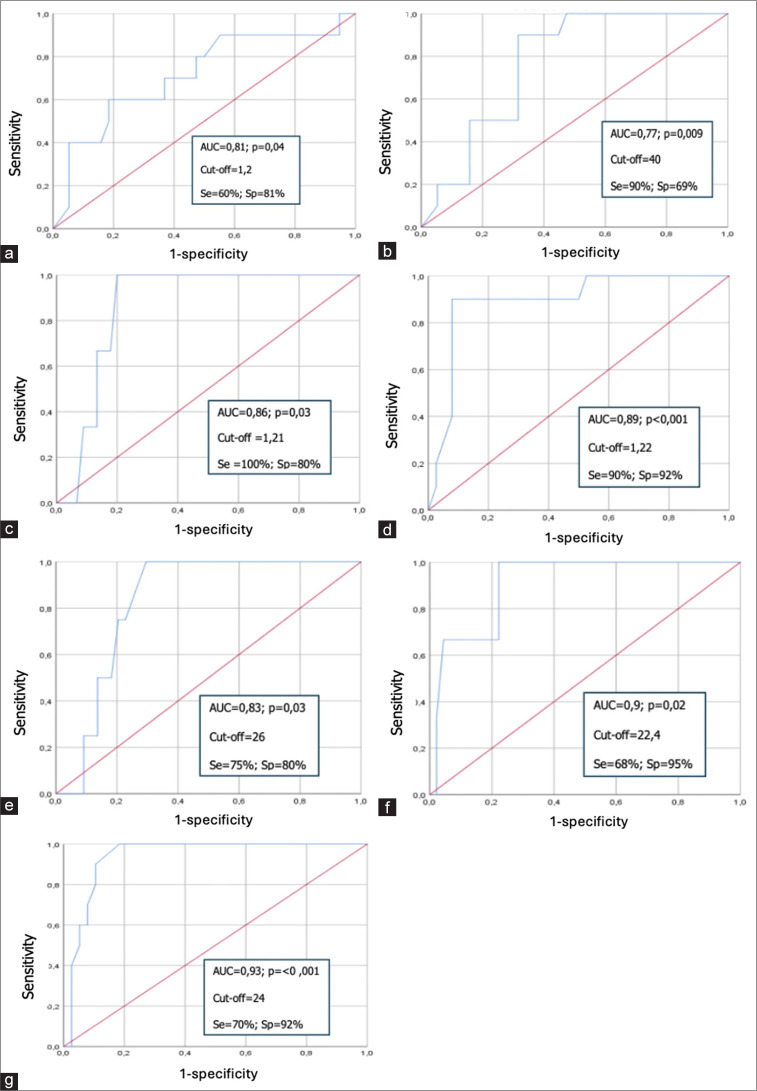
Results: Post-operative SV and MV significantly increased compared to pre-operative values (P = 0.008 and P = 0.037, respectively), while PI and DV remained stable. Pre-operative elevated PI and decreased DV were significantly associated with post-operative complications, including delayed awakening and ischemia. Postoperative PI predicted ischemia with an area under the curve (AUC) of 0.86 and delayed awakening with an AUC of 0.89. Lower DV values were predictive of seizures, ischemia, and delayed awakening. Elevated PI and reduced DV correlated with longer intensive care unit stays.
Conclusion: TCCD is a valuable, non-invasive tool for early identification of patients at risk for post-operative complications following craniotomy for tumor resection. Monitoring PI and DV may guide post-operative management and improve outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


