Gretchen L Sacha, Abhijit Duggal, Anita J Reddy, Lu Wang, Seth R Bauer
{"title":"抗利尿激素起始时间与脓毒性休克住院死亡率:大型公共数据库的观察性研究","authors":"Gretchen L Sacha, Abhijit Duggal, Anita J Reddy, Lu Wang, Seth R Bauer","doi":"10.1097/CCE.0000000000001284","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Vasopressin is used in one-third of patients with septic shock to augment hemodynamics and reduce overall catecholamine exposure. However, the optimal clinical context in which to initiate vasopressin is unknown.</p><p><strong>Objectives: </strong>To determine the association between norepinephrine-equivalent dose, lactate concentration, and time duration from shock onset at vasopressin initiation with in-hospital mortality.</p><p><strong>Design, setting, and participants: </strong>Retrospective, observational evaluation utilizing Medical Information Mart for Intensive Care-IV and electronic ICU Collaborative Research Database databases of adult patients with septic shock based on modified Sepsis-3 criteria receiving continuous infusion catecholamines.</p><p><strong>Main outcomes and measures: </strong>The associations of norepinephrine-equivalent dose, lactate concentration, and time duration from shock onset at vasopressin initiation with in-hospital mortality were evaluated with multivariable regression models.</p><p><strong>Results: </strong>In total, 1409 patients from 209 hospitals were included. At vasopressin initiation patients had a median (interquartile range) norepinephrine-equivalent dose 28.4 µg/min (16.4-42.6 µg/min), lactate concentration 3.7 mmol/L (2.5-6.2 mmol/L), and 5.6 hours (2.0-13.5 hr) had elapsed since shock onset. All three variables of interest were associated with in-hospital mortality. Three restricted cubic spline knots were identified where the relationship between norepinephrine-equivalent dose and in-hospital mortality changed substantially: 9, 28, and 72 µg/min. The odds of in-hospital mortality increased by 90% and 3.9-fold when comparing vasopressin initiation at norepinephrine-equivalent doses of 28 µg/min and 72 µg/min to 9 µg/min, respectively (adjusted odds ratio [OR], 1.90 [95% CI, 1.49-2.41] and 3.93 [95% CI, 2.74-5.64]). The odds of in-hospital mortality increased by 16% for every mmol/L in the lactate concentration at vasopressin initiation (adjusted OR, 1.16 [95% CI, 1.11-1.21]). Finally, the odds of in-hospital mortality increased by 3% for every hour in the time duration from shock onset to vasopressin initiation (adjusted OR, 1.03 [95% CI, 1.01-1.04]).</p><p><strong>Conclusions and relevance: </strong>Earlier adjunctive vasopressin initiation may decrease mortality in patients with septic shock.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 9","pages":"e1284"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377302/pdf/","citationCount":"0","resultStr":"{\"title\":\"Vasopressin Initiation Timing and In-Hospital Mortality in Septic Shock: An Observational Study of Large Public Databases.\",\"authors\":\"Gretchen L Sacha, Abhijit Duggal, Anita J Reddy, Lu Wang, Seth R Bauer\",\"doi\":\"10.1097/CCE.0000000000001284\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Vasopressin is used in one-third of patients with septic shock to augment hemodynamics and reduce overall catecholamine exposure. However, the optimal clinical context in which to initiate vasopressin is unknown.</p><p><strong>Objectives: </strong>To determine the association between norepinephrine-equivalent dose, lactate concentration, and time duration from shock onset at vasopressin initiation with in-hospital mortality.</p><p><strong>Design, setting, and participants: </strong>Retrospective, observational evaluation utilizing Medical Information Mart for Intensive Care-IV and electronic ICU Collaborative Research Database databases of adult patients with septic shock based on modified Sepsis-3 criteria receiving continuous infusion catecholamines.</p><p><strong>Main outcomes and measures: </strong>The associations of norepinephrine-equivalent dose, lactate concentration, and time duration from shock onset at vasopressin initiation with in-hospital mortality were evaluated with multivariable regression models.</p><p><strong>Results: </strong>In total, 1409 patients from 209 hospitals were included. At vasopressin initiation patients had a median (interquartile range) norepinephrine-equivalent dose 28.4 µg/min (16.4-42.6 µg/min), lactate concentration 3.7 mmol/L (2.5-6.2 mmol/L), and 5.6 hours (2.0-13.5 hr) had elapsed since shock onset. All three variables of interest were associated with in-hospital mortality. Three restricted cubic spline knots were identified where the relationship between norepinephrine-equivalent dose and in-hospital mortality changed substantially: 9, 28, and 72 µg/min. The odds of in-hospital mortality increased by 90% and 3.9-fold when comparing vasopressin initiation at norepinephrine-equivalent doses of 28 µg/min and 72 µg/min to 9 µg/min, respectively (adjusted odds ratio [OR], 1.90 [95% CI, 1.49-2.41] and 3.93 [95% CI, 2.74-5.64]). The odds of in-hospital mortality increased by 16% for every mmol/L in the lactate concentration at vasopressin initiation (adjusted OR, 1.16 [95% CI, 1.11-1.21]). Finally, the odds of in-hospital mortality increased by 3% for every hour in the time duration from shock onset to vasopressin initiation (adjusted OR, 1.03 [95% CI, 1.01-1.04]).</p><p><strong>Conclusions and relevance: </strong>Earlier adjunctive vasopressin initiation may decrease mortality in patients with septic shock.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 9\",\"pages\":\"e1284\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377302/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001284\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001284","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Vasopressin Initiation Timing and In-Hospital Mortality in Septic Shock: An Observational Study of Large Public Databases.
Importance: Vasopressin is used in one-third of patients with septic shock to augment hemodynamics and reduce overall catecholamine exposure. However, the optimal clinical context in which to initiate vasopressin is unknown.
Objectives: To determine the association between norepinephrine-equivalent dose, lactate concentration, and time duration from shock onset at vasopressin initiation with in-hospital mortality.
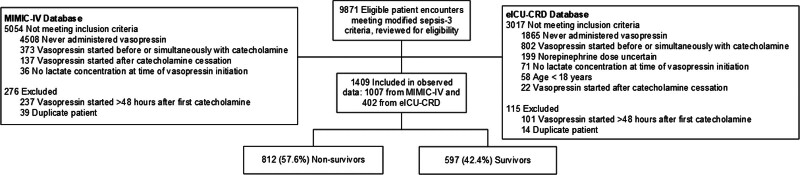
Design, setting, and participants: Retrospective, observational evaluation utilizing Medical Information Mart for Intensive Care-IV and electronic ICU Collaborative Research Database databases of adult patients with septic shock based on modified Sepsis-3 criteria receiving continuous infusion catecholamines.
Main outcomes and measures: The associations of norepinephrine-equivalent dose, lactate concentration, and time duration from shock onset at vasopressin initiation with in-hospital mortality were evaluated with multivariable regression models.
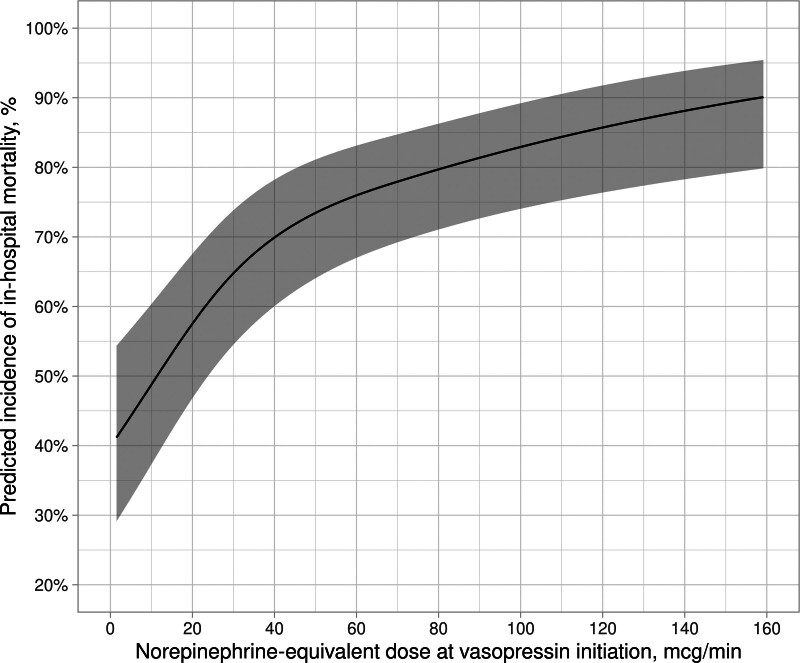
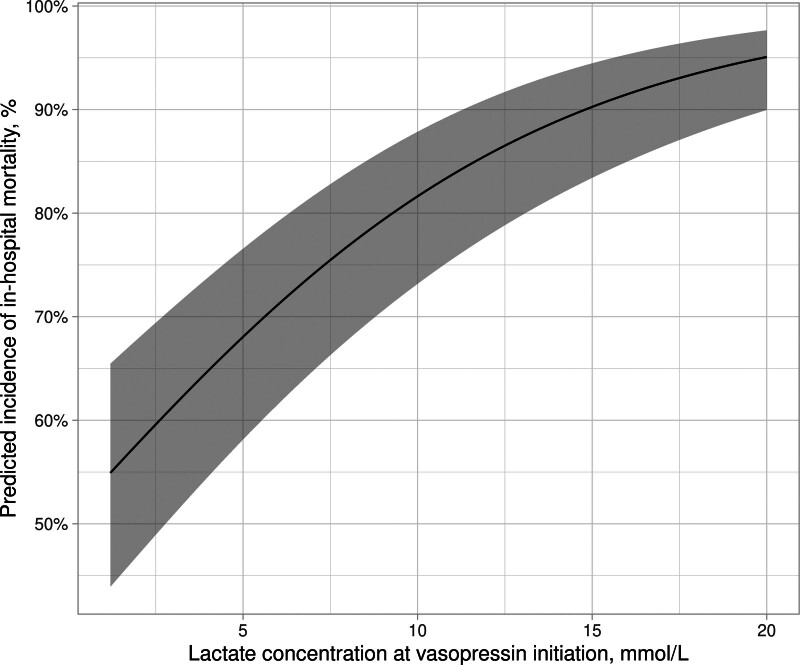
Results: In total, 1409 patients from 209 hospitals were included. At vasopressin initiation patients had a median (interquartile range) norepinephrine-equivalent dose 28.4 µg/min (16.4-42.6 µg/min), lactate concentration 3.7 mmol/L (2.5-6.2 mmol/L), and 5.6 hours (2.0-13.5 hr) had elapsed since shock onset. All three variables of interest were associated with in-hospital mortality. Three restricted cubic spline knots were identified where the relationship between norepinephrine-equivalent dose and in-hospital mortality changed substantially: 9, 28, and 72 µg/min. The odds of in-hospital mortality increased by 90% and 3.9-fold when comparing vasopressin initiation at norepinephrine-equivalent doses of 28 µg/min and 72 µg/min to 9 µg/min, respectively (adjusted odds ratio [OR], 1.90 [95% CI, 1.49-2.41] and 3.93 [95% CI, 2.74-5.64]). The odds of in-hospital mortality increased by 16% for every mmol/L in the lactate concentration at vasopressin initiation (adjusted OR, 1.16 [95% CI, 1.11-1.21]). Finally, the odds of in-hospital mortality increased by 3% for every hour in the time duration from shock onset to vasopressin initiation (adjusted OR, 1.03 [95% CI, 1.01-1.04]).
Conclusions and relevance: Earlier adjunctive vasopressin initiation may decrease mortality in patients with septic shock.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


