Luca Molinari, Mark A Tidswell, Ali Al-Khafaji, Danielle Davison, Claude Galphin, Esha Kamaluddin, Debra M Foster, John A Kellum
{"title":"感染性休克的器官衰竭、内毒素活性和死亡率。","authors":"Luca Molinari, Mark A Tidswell, Ali Al-Khafaji, Danielle Davison, Claude Galphin, Esha Kamaluddin, Debra M Foster, John A Kellum","doi":"10.1097/CCE.0000000000001308","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The relationship between endotoxin activity, organ failure, and mortality is not well understood.</p><p><strong>Objective: </strong>To test whether the combination of endotoxin activity and organ failure identifies patients at higher risk of death from sepsis and determine the relationship to previously described sepsis phenotypes.</p><p><strong>Design, setting, and participants: </strong>Prospective observational study in four ICUs enrolling critically ill patients with septic shock.</p><p><strong>Main outcomes and measures: </strong>Endotoxin activity assay (EAA) results, Sequential Organ Failure Assessment (SOFA), and multiple organ dysfunction (MODS) and 28-day mortality.</p><p><strong>Results: </strong>We enrolled 90 patients aged 25-95 years and set an EAA cutoff of greater than or equal to 0.6 together with SOFA greater than 11 or MODS greater than 9 to define endotoxic septic shock (ESS). At baseline mean EAA was 0.64 (sd = 0.19), whereas mean SOFA and MODS were 10.3 (sd 3.2) and 5.8 (sd 3.1), respectively. EAA greater than or equal to 0.6 and SOFA greater than 11 were present in 20 patients (23.3%) and these patients had 60% mortality. EAA greater than or equal to 0.6 and SOFA less than or equal to 11 occurred in 31 (36.0%) with mortality 12.9%. Of the 35 remaining patients with EAA less than 0.6, 29 (33.7%) had SOFA less than or equal to 11 and 5 of them (17.2%) died. Only six patients (7.0%) had EAA less than 0.6 and SOFA greater than 11 and none died (p < 0.001). All patients with MODS greater than 9 also had EAA greater than or equal to 0.6 (12 patients) with 75% mortality. EAA greater than or equal to 0.6 with MODS less than or equal to 9 occurred in 39 patients with 17.9% mortality (p < 0.001). ESS (EAA ≥ 0.6 together with SOFA > 11 or MODS > 9) occurred in 21 patients and they had significantly higher mortality (57.1% vs. 15.9%, p < 0.001) compared with non-ESS, with a relative risk for death of 3.58 (95% CI, 1.86-6.91). Among ESS patients, 7 (33.3%) had δ phenotype, whereas only 4 (5.8%) had δ among non-ESS (p = 0.001).</p><p><strong>Conclusions and relevance: </strong>ESS compromises patients with the highest mortality rate from sepsis. Such patients are most appropriate for trials testing anti-endotoxin therapy for improving survival.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 9","pages":"e1308"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398369/pdf/","citationCount":"0","resultStr":"{\"title\":\"Organ Failure, Endotoxin Activity, and Mortality in Septic Shock.\",\"authors\":\"Luca Molinari, Mark A Tidswell, Ali Al-Khafaji, Danielle Davison, Claude Galphin, Esha Kamaluddin, Debra M Foster, John A Kellum\",\"doi\":\"10.1097/CCE.0000000000001308\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>The relationship between endotoxin activity, organ failure, and mortality is not well understood.</p><p><strong>Objective: </strong>To test whether the combination of endotoxin activity and organ failure identifies patients at higher risk of death from sepsis and determine the relationship to previously described sepsis phenotypes.</p><p><strong>Design, setting, and participants: </strong>Prospective observational study in four ICUs enrolling critically ill patients with septic shock.</p><p><strong>Main outcomes and measures: </strong>Endotoxin activity assay (EAA) results, Sequential Organ Failure Assessment (SOFA), and multiple organ dysfunction (MODS) and 28-day mortality.</p><p><strong>Results: </strong>We enrolled 90 patients aged 25-95 years and set an EAA cutoff of greater than or equal to 0.6 together with SOFA greater than 11 or MODS greater than 9 to define endotoxic septic shock (ESS). At baseline mean EAA was 0.64 (sd = 0.19), whereas mean SOFA and MODS were 10.3 (sd 3.2) and 5.8 (sd 3.1), respectively. EAA greater than or equal to 0.6 and SOFA greater than 11 were present in 20 patients (23.3%) and these patients had 60% mortality. EAA greater than or equal to 0.6 and SOFA less than or equal to 11 occurred in 31 (36.0%) with mortality 12.9%. Of the 35 remaining patients with EAA less than 0.6, 29 (33.7%) had SOFA less than or equal to 11 and 5 of them (17.2%) died. Only six patients (7.0%) had EAA less than 0.6 and SOFA greater than 11 and none died (p < 0.001). All patients with MODS greater than 9 also had EAA greater than or equal to 0.6 (12 patients) with 75% mortality. EAA greater than or equal to 0.6 with MODS less than or equal to 9 occurred in 39 patients with 17.9% mortality (p < 0.001). ESS (EAA ≥ 0.6 together with SOFA > 11 or MODS > 9) occurred in 21 patients and they had significantly higher mortality (57.1% vs. 15.9%, p < 0.001) compared with non-ESS, with a relative risk for death of 3.58 (95% CI, 1.86-6.91). Among ESS patients, 7 (33.3%) had δ phenotype, whereas only 4 (5.8%) had δ among non-ESS (p = 0.001).</p><p><strong>Conclusions and relevance: </strong>ESS compromises patients with the highest mortality rate from sepsis. Such patients are most appropriate for trials testing anti-endotoxin therapy for improving survival.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 9\",\"pages\":\"e1308\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-08-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398369/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001308\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001308","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Organ Failure, Endotoxin Activity, and Mortality in Septic Shock.
Importance: The relationship between endotoxin activity, organ failure, and mortality is not well understood.
Objective: To test whether the combination of endotoxin activity and organ failure identifies patients at higher risk of death from sepsis and determine the relationship to previously described sepsis phenotypes.
Design, setting, and participants: Prospective observational study in four ICUs enrolling critically ill patients with septic shock.
Main outcomes and measures: Endotoxin activity assay (EAA) results, Sequential Organ Failure Assessment (SOFA), and multiple organ dysfunction (MODS) and 28-day mortality.
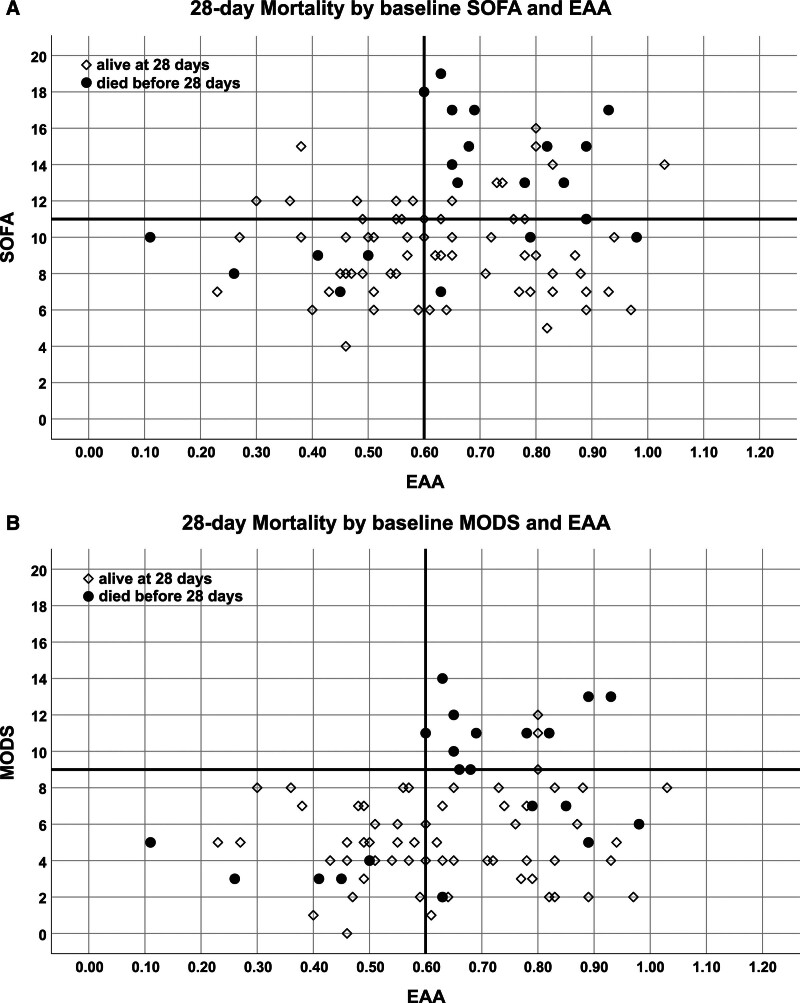
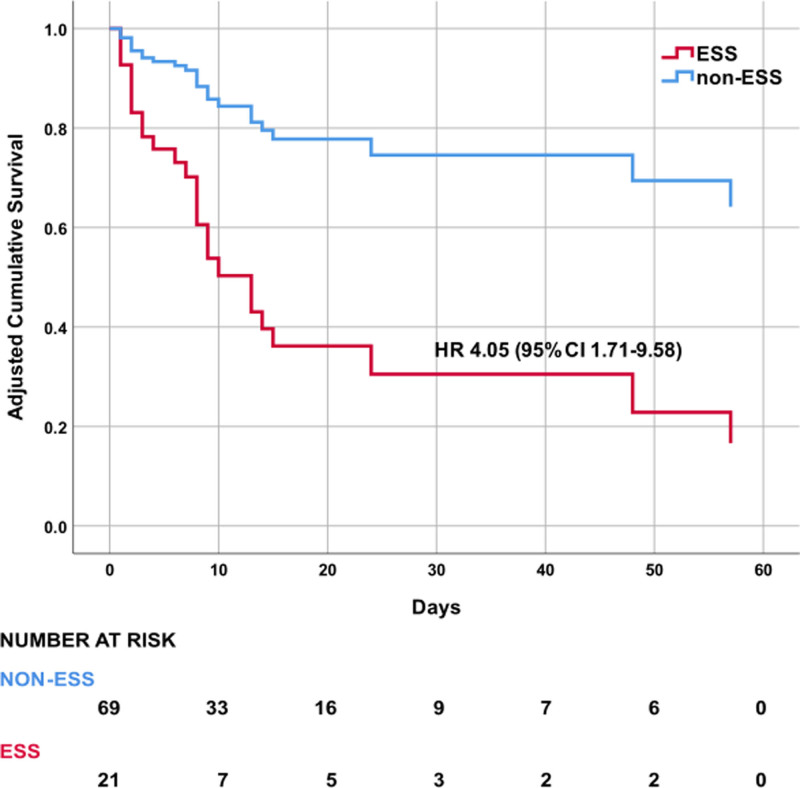
Results: We enrolled 90 patients aged 25-95 years and set an EAA cutoff of greater than or equal to 0.6 together with SOFA greater than 11 or MODS greater than 9 to define endotoxic septic shock (ESS). At baseline mean EAA was 0.64 (sd = 0.19), whereas mean SOFA and MODS were 10.3 (sd 3.2) and 5.8 (sd 3.1), respectively. EAA greater than or equal to 0.6 and SOFA greater than 11 were present in 20 patients (23.3%) and these patients had 60% mortality. EAA greater than or equal to 0.6 and SOFA less than or equal to 11 occurred in 31 (36.0%) with mortality 12.9%. Of the 35 remaining patients with EAA less than 0.6, 29 (33.7%) had SOFA less than or equal to 11 and 5 of them (17.2%) died. Only six patients (7.0%) had EAA less than 0.6 and SOFA greater than 11 and none died (p < 0.001). All patients with MODS greater than 9 also had EAA greater than or equal to 0.6 (12 patients) with 75% mortality. EAA greater than or equal to 0.6 with MODS less than or equal to 9 occurred in 39 patients with 17.9% mortality (p < 0.001). ESS (EAA ≥ 0.6 together with SOFA > 11 or MODS > 9) occurred in 21 patients and they had significantly higher mortality (57.1% vs. 15.9%, p < 0.001) compared with non-ESS, with a relative risk for death of 3.58 (95% CI, 1.86-6.91). Among ESS patients, 7 (33.3%) had δ phenotype, whereas only 4 (5.8%) had δ among non-ESS (p = 0.001).
Conclusions and relevance: ESS compromises patients with the highest mortality rate from sepsis. Such patients are most appropriate for trials testing anti-endotoxin therapy for improving survival.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


