Camila Braganca Xavier, Clark R Andersen, JoAnn Lim, Julian H Slade, Stacie A Bean, Lei Kang, Hung Le, Apostolia M Tsimberidou, Aung Naing, David S Hong, Ecaterina E Dumbrava, Jordi Rodon Ahnert, Paula R Pohlmann, Sarina A Piha-Paul, Stephane Champiat, Timothy A Yap, Tin-Yun Tang, Funda Meric-Bernstam, Siqing Fu
{"title":"在免疫治疗试验中调节实体瘤患者的治疗结果:来自1期单位的药物相互作用分析。","authors":"Camila Braganca Xavier, Clark R Andersen, JoAnn Lim, Julian H Slade, Stacie A Bean, Lei Kang, Hung Le, Apostolia M Tsimberidou, Aung Naing, David S Hong, Ecaterina E Dumbrava, Jordi Rodon Ahnert, Paula R Pohlmann, Sarina A Piha-Paul, Stephane Champiat, Timothy A Yap, Tin-Yun Tang, Funda Meric-Bernstam, Siqing Fu","doi":"10.1158/2767-9764.CRC-25-0033","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Concurrent use of medications can modulate the effectiveness of immunotherapy. Although this interaction is well documented for immune checkpoint inhibitors, whether this occurs with new experimental compounds has not been evaluated.</p><p><strong>Patients and methods: </strong>A computerized data extraction tool was used to collect clinical data and identify the prescription of a predefined set of medications within 30 days of immunotherapy infusion in the Department of Investigational Cancer Therapeutics at the University of Texas MD Anderson Cancer Center. The primary endpoints were median overall survival (OS) and progression-free survival. Tumor responses were assessed using RECIST.</p><p><strong>Results: </strong>We identified 897 patients. The most prevalent tumor types were colorectal (24.5%), head and neck (10.5%), and pancreatic (9.4%). The immunotherapy administered consisted of monoclonal antibodies and fusion proteins (64.7%), immune modulators (IM; 20.8%), combinations of IMs and antibodies (9.2%), and oncolytic viruses and cancer vaccines (5.3%). The most frequently prescribed drugs were narcotics (70.5%), antiemetics (49.1%), antihistamines (34.6%), antibiotics (31.2%), and proton pump inhibitors (PPI; 28.7%). Patients receiving antihistamines exhibited increased rates of stable disease and partial response (χ2 8.48; P = 0.014) on the IMs and antibodies combination. The benefit of antihistamines was confirmed in a multivariate analysis of OS [HR, 0.752 (95% CI, 0.603-0.938); P = 0.012]. For patients with colorectal cancer, PPI use was associated with shortened survival, with a median OS of 5.2 months with PPI use and 8.6 months without it (P < 0.001).</p><p><strong>Conclusions: </strong>Our findings highlight the need for strategies to guide concurrent medication choices for patients receiving immunotherapy in early-phase trials.</p><p><strong>Significance: </strong>Concurrent administration of antihistamines correlates with enhanced survival in patients receiving experimental immunotherapy for cancer. Conversely, PPI use diminishes survival in patients with colorectal cancer. These findings highlight how tumor immunogenicity and drug interactions can modulate response and survival outcomes, offering new insights to optimize investigational immunotherapy.</p>","PeriodicalId":72516,"journal":{"name":"Cancer research communications","volume":" ","pages":"1631-1641"},"PeriodicalIF":3.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12434680/pdf/","citationCount":"0","resultStr":"{\"title\":\"Modulating Treatment Outcomes of Patients with Solid Tumors in Immunotherapy Trials: A Drug Interaction Analysis from a Phase I Unit.\",\"authors\":\"Camila Braganca Xavier, Clark R Andersen, JoAnn Lim, Julian H Slade, Stacie A Bean, Lei Kang, Hung Le, Apostolia M Tsimberidou, Aung Naing, David S Hong, Ecaterina E Dumbrava, Jordi Rodon Ahnert, Paula R Pohlmann, Sarina A Piha-Paul, Stephane Champiat, Timothy A Yap, Tin-Yun Tang, Funda Meric-Bernstam, Siqing Fu\",\"doi\":\"10.1158/2767-9764.CRC-25-0033\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Concurrent use of medications can modulate the effectiveness of immunotherapy. Although this interaction is well documented for immune checkpoint inhibitors, whether this occurs with new experimental compounds has not been evaluated.</p><p><strong>Patients and methods: </strong>A computerized data extraction tool was used to collect clinical data and identify the prescription of a predefined set of medications within 30 days of immunotherapy infusion in the Department of Investigational Cancer Therapeutics at the University of Texas MD Anderson Cancer Center. The primary endpoints were median overall survival (OS) and progression-free survival. Tumor responses were assessed using RECIST.</p><p><strong>Results: </strong>We identified 897 patients. The most prevalent tumor types were colorectal (24.5%), head and neck (10.5%), and pancreatic (9.4%). The immunotherapy administered consisted of monoclonal antibodies and fusion proteins (64.7%), immune modulators (IM; 20.8%), combinations of IMs and antibodies (9.2%), and oncolytic viruses and cancer vaccines (5.3%). The most frequently prescribed drugs were narcotics (70.5%), antiemetics (49.1%), antihistamines (34.6%), antibiotics (31.2%), and proton pump inhibitors (PPI; 28.7%). Patients receiving antihistamines exhibited increased rates of stable disease and partial response (χ2 8.48; P = 0.014) on the IMs and antibodies combination. The benefit of antihistamines was confirmed in a multivariate analysis of OS [HR, 0.752 (95% CI, 0.603-0.938); P = 0.012]. For patients with colorectal cancer, PPI use was associated with shortened survival, with a median OS of 5.2 months with PPI use and 8.6 months without it (P < 0.001).</p><p><strong>Conclusions: </strong>Our findings highlight the need for strategies to guide concurrent medication choices for patients receiving immunotherapy in early-phase trials.</p><p><strong>Significance: </strong>Concurrent administration of antihistamines correlates with enhanced survival in patients receiving experimental immunotherapy for cancer. Conversely, PPI use diminishes survival in patients with colorectal cancer. These findings highlight how tumor immunogenicity and drug interactions can modulate response and survival outcomes, offering new insights to optimize investigational immunotherapy.</p>\",\"PeriodicalId\":72516,\"journal\":{\"name\":\"Cancer research communications\",\"volume\":\" \",\"pages\":\"1631-1641\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12434680/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer research communications\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1158/2767-9764.CRC-25-0033\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer research communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1158/2767-9764.CRC-25-0033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Modulating Treatment Outcomes of Patients with Solid Tumors in Immunotherapy Trials: A Drug Interaction Analysis from a Phase I Unit.
Purpose: Concurrent use of medications can modulate the effectiveness of immunotherapy. Although this interaction is well documented for immune checkpoint inhibitors, whether this occurs with new experimental compounds has not been evaluated.
Patients and methods: A computerized data extraction tool was used to collect clinical data and identify the prescription of a predefined set of medications within 30 days of immunotherapy infusion in the Department of Investigational Cancer Therapeutics at the University of Texas MD Anderson Cancer Center. The primary endpoints were median overall survival (OS) and progression-free survival. Tumor responses were assessed using RECIST.
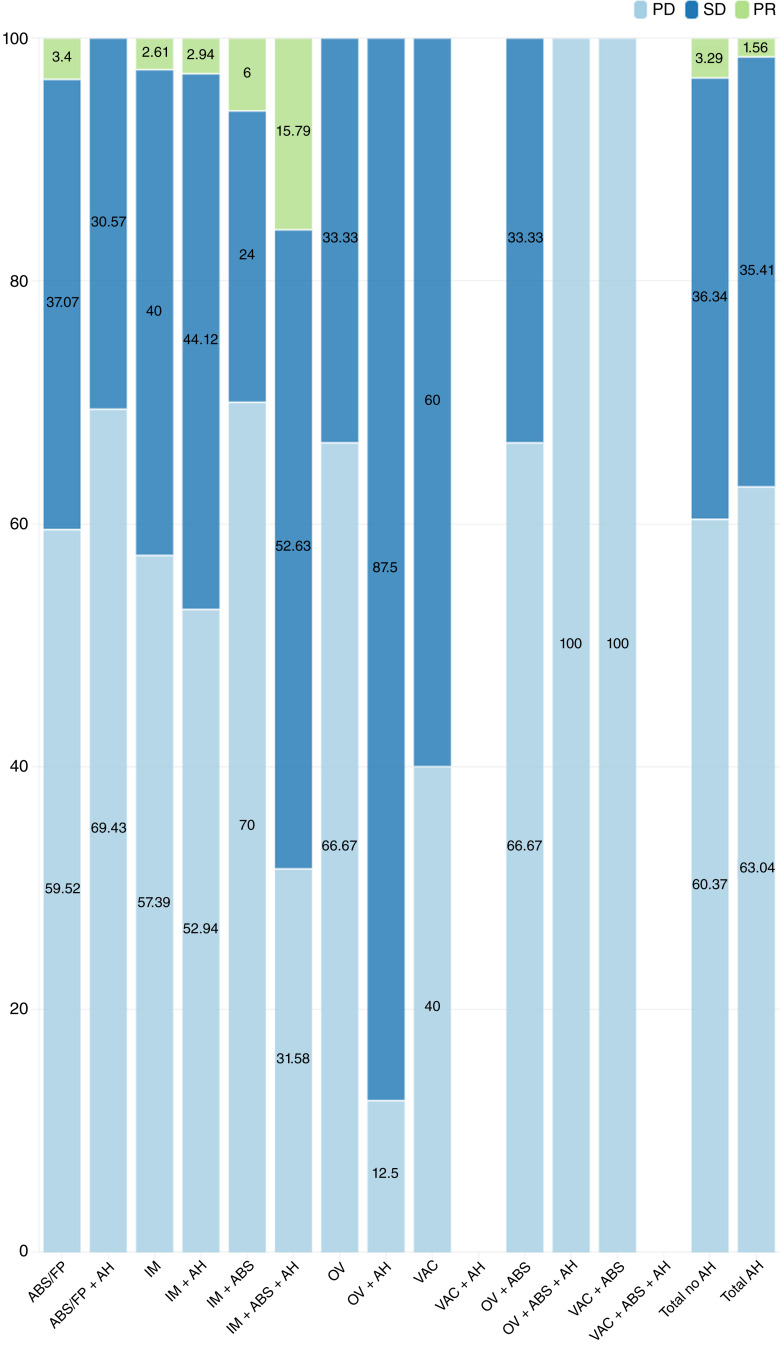
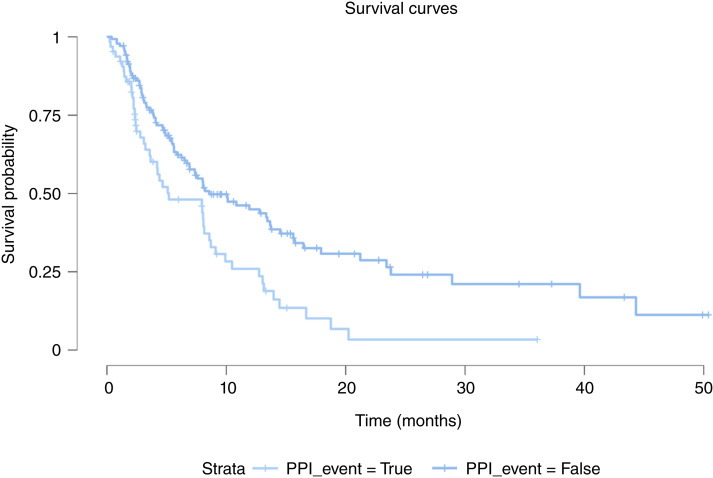
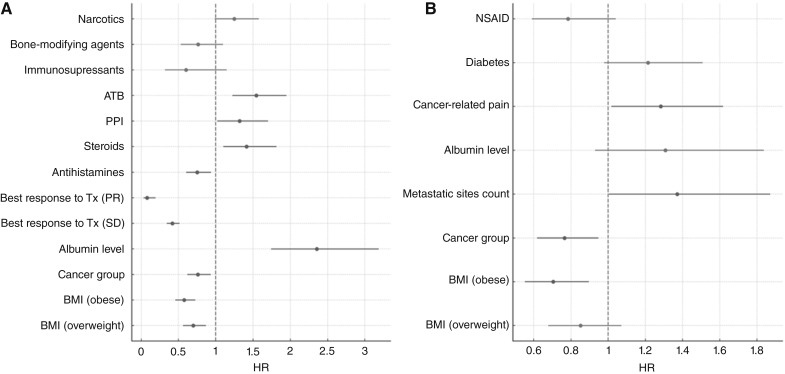
Results: We identified 897 patients. The most prevalent tumor types were colorectal (24.5%), head and neck (10.5%), and pancreatic (9.4%). The immunotherapy administered consisted of monoclonal antibodies and fusion proteins (64.7%), immune modulators (IM; 20.8%), combinations of IMs and antibodies (9.2%), and oncolytic viruses and cancer vaccines (5.3%). The most frequently prescribed drugs were narcotics (70.5%), antiemetics (49.1%), antihistamines (34.6%), antibiotics (31.2%), and proton pump inhibitors (PPI; 28.7%). Patients receiving antihistamines exhibited increased rates of stable disease and partial response (χ2 8.48; P = 0.014) on the IMs and antibodies combination. The benefit of antihistamines was confirmed in a multivariate analysis of OS [HR, 0.752 (95% CI, 0.603-0.938); P = 0.012]. For patients with colorectal cancer, PPI use was associated with shortened survival, with a median OS of 5.2 months with PPI use and 8.6 months without it (P < 0.001).
Conclusions: Our findings highlight the need for strategies to guide concurrent medication choices for patients receiving immunotherapy in early-phase trials.
Significance: Concurrent administration of antihistamines correlates with enhanced survival in patients receiving experimental immunotherapy for cancer. Conversely, PPI use diminishes survival in patients with colorectal cancer. These findings highlight how tumor immunogenicity and drug interactions can modulate response and survival outcomes, offering new insights to optimize investigational immunotherapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


