Dimitrios Giannis, Ruby Zhao, Luis Fernandez, Nicole Nikolov, Christina Sneed, Patrick Kiarie, Andrew Miele, Martine A Louis, Nageswara Rao Mandava
{"title":"紧急非心脏手术术后心房颤动:一项为期十年的重症监护病房回顾性研究的危险因素和结果。","authors":"Dimitrios Giannis, Ruby Zhao, Luis Fernandez, Nicole Nikolov, Christina Sneed, Patrick Kiarie, Andrew Miele, Martine A Louis, Nageswara Rao Mandava","doi":"10.5492/wjccm.v14.i3.102991","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atrial fibrillation (AF) represents a common arrhythmia with significant implications and may occur pre-, intra-, or postoperatively (POAF). After cardiac surgery POAF occurs in approximately 30% of patients, while non-cardiac/non-thoracic surgery has a reported incidence between 0.4% to 15%, with new onset POAF occurring at a rate of 0.4% to 3%. While AF has been extensively studied, it has not been well described in emergent non-cardiac surgery associated with increased surgical stress in an intensive care unit setting (ICU).</p><p><strong>Aim: </strong>To investigate the incidence/predictors of POAF in emergent non-cardiac surgery and its associations with postoperative outcomes in the ICU.</p><p><strong>Methods: </strong>This retrospective study included patients ≥ 18 years who underwent exploratory laparotomy or lower extremity amputation between October 2012 and September 2023 and were admitted in the ICU. Data of interest included occurrence of POAF, demographic characteristics, comorbidities, laboratory values, administered fluids, medications, and postoperative outcomes. Statistical analyses consisted of identifying predictors of POAF and associations of POAF with outcomes of interest.</p><p><strong>Results: </strong>A total of 347 ICU patients were included, 16.4% had a history of AF, 13.0% developed POAF, and 7.9% developed new-onset POAF. Patients with new-onset POAF were older (79.6 ± 9.1 <i>vs</i> 68.1 ± 14.8 years, < 0.001), of white race (47.8% <i>vs</i> 28.8, <i>P</i> < 0.001), hypertensive (87.0% <i>vs</i> 71.2%, <i>P =</i> 0.011), had longer ICU length of stay (ICU-LOS) (13.4 <i>vs</i> 6.7 days, <i>P =</i> 0.042), higher mortality (43.5% <i>vs</i> 17.6%, <i>P =</i> 0.016) and higher rate of cardiac arrest (34.8% <i>vs</i> 14.6%, <i>P =</i> 0.005) compared to patients without new-onset POAF. Multivariable analysis revealed increased POAF risk with advanced age (OR = 1.06; 95%CI: 1.02-1.10, <i>P =</i> 0.005), white race (OR = 2.85; 95%CI: 1.26-6.76, <i>P =</i> 0.014), high intraoperative fluid (OR > 1; 95%CI: 1.00-1.00, <i>P =</i> 0.018), and longer ICU-LOS (OR = 1.04; 95%CI: 1.00-1.08, <i>P =</i> 0.023). After adjusting for demographics, new onset POAF significantly predicted mortality (OR = 3.07; 95%CI: 1.14-8.01, <i>P =</i> 0.022).</p><p><strong>Conclusion: </strong>POAF was associated with prolonged ICU-LOS, white race, and high intraoperative fluid. New-onset POAF was associated with increased risk of cardiac arrest and death in critically ill patients.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"14 3","pages":"102991"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304932/pdf/","citationCount":"0","resultStr":"{\"title\":\"Postoperative atrial fibrillation in emergent non-cardiac surgery: Risk factors and outcomes from a ten-year intensive-care unit retrospective study.\",\"authors\":\"Dimitrios Giannis, Ruby Zhao, Luis Fernandez, Nicole Nikolov, Christina Sneed, Patrick Kiarie, Andrew Miele, Martine A Louis, Nageswara Rao Mandava\",\"doi\":\"10.5492/wjccm.v14.i3.102991\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Atrial fibrillation (AF) represents a common arrhythmia with significant implications and may occur pre-, intra-, or postoperatively (POAF). After cardiac surgery POAF occurs in approximately 30% of patients, while non-cardiac/non-thoracic surgery has a reported incidence between 0.4% to 15%, with new onset POAF occurring at a rate of 0.4% to 3%. While AF has been extensively studied, it has not been well described in emergent non-cardiac surgery associated with increased surgical stress in an intensive care unit setting (ICU).</p><p><strong>Aim: </strong>To investigate the incidence/predictors of POAF in emergent non-cardiac surgery and its associations with postoperative outcomes in the ICU.</p><p><strong>Methods: </strong>This retrospective study included patients ≥ 18 years who underwent exploratory laparotomy or lower extremity amputation between October 2012 and September 2023 and were admitted in the ICU. Data of interest included occurrence of POAF, demographic characteristics, comorbidities, laboratory values, administered fluids, medications, and postoperative outcomes. Statistical analyses consisted of identifying predictors of POAF and associations of POAF with outcomes of interest.</p><p><strong>Results: </strong>A total of 347 ICU patients were included, 16.4% had a history of AF, 13.0% developed POAF, and 7.9% developed new-onset POAF. Patients with new-onset POAF were older (79.6 ± 9.1 <i>vs</i> 68.1 ± 14.8 years, < 0.001), of white race (47.8% <i>vs</i> 28.8, <i>P</i> < 0.001), hypertensive (87.0% <i>vs</i> 71.2%, <i>P =</i> 0.011), had longer ICU length of stay (ICU-LOS) (13.4 <i>vs</i> 6.7 days, <i>P =</i> 0.042), higher mortality (43.5% <i>vs</i> 17.6%, <i>P =</i> 0.016) and higher rate of cardiac arrest (34.8% <i>vs</i> 14.6%, <i>P =</i> 0.005) compared to patients without new-onset POAF. Multivariable analysis revealed increased POAF risk with advanced age (OR = 1.06; 95%CI: 1.02-1.10, <i>P =</i> 0.005), white race (OR = 2.85; 95%CI: 1.26-6.76, <i>P =</i> 0.014), high intraoperative fluid (OR > 1; 95%CI: 1.00-1.00, <i>P =</i> 0.018), and longer ICU-LOS (OR = 1.04; 95%CI: 1.00-1.08, <i>P =</i> 0.023). After adjusting for demographics, new onset POAF significantly predicted mortality (OR = 3.07; 95%CI: 1.14-8.01, <i>P =</i> 0.022).</p><p><strong>Conclusion: </strong>POAF was associated with prolonged ICU-LOS, white race, and high intraoperative fluid. New-onset POAF was associated with increased risk of cardiac arrest and death in critically ill patients.</p>\",\"PeriodicalId\":66959,\"journal\":{\"name\":\"世界危重病急救学杂志(英文版)\",\"volume\":\"14 3\",\"pages\":\"102991\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304932/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"世界危重病急救学杂志(英文版)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5492/wjccm.v14.i3.102991\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5492/wjccm.v14.i3.102991","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:心房颤动(AF)是一种具有重要意义的常见心律失常,可能发生在手术前、手术中或手术后。心脏手术后POAF发生在大约30%的患者中,而非心脏/非胸外科手术的发生率在0.4%至15%之间,新发POAF发生率为0.4%至3%。虽然对房颤进行了广泛的研究,但在重症监护病房(ICU)中与手术压力增加相关的紧急非心脏手术中,房颤尚未得到很好的描述。目的:探讨急诊非心脏手术中POAF的发生率/预测因素及其与ICU术后预后的关系。方法:本回顾性研究纳入2012年10月至2023年9月在ICU住院的≥18岁的剖腹探查或下肢截肢患者。感兴趣的数据包括POAF的发生、人口学特征、合并症、实验室值、给予的液体、药物和术后结果。统计分析包括确定POAF的预测因素以及POAF与相关结果的关联。结果:共纳入347例ICU患者,有房颤病史的占16.4%,发生POAF的占13.0%,新发POAF的占7.9%。与非新发POAF患者相比,新发POAF患者年龄较大(79.6±9.1岁vs 68.1±14.8岁,< 0.001)、白人(47.8% vs 28.8岁,P < 0.001)、高血压(87.0% vs 71.2%, P = 0.011)、ICU住院时间较长(13.4 vs 6.7天,P = 0.042)、死亡率较高(43.5% vs 17.6%, P = 0.016)、心脏骤停率较高(34.8% vs 14.6%, P = 0.005)。多变量分析显示,高龄(OR = 1.06; 95%CI: 1.02-1.10, P = 0.005)、白种人(OR = 2.85; 95%CI: 1.26-6.76, P = 0.014)、术中积液高(OR = bbb1; 95%CI: 1.00-1.00, P = 0.018)、ICU-LOS较长(OR = 1.04; 95%CI: 1.00-1.08, P = 0.023)增加了POAF的风险。调整人口统计学因素后,新发POAF显著预测死亡率(OR = 3.07; 95%CI: 1.14-8.01, P = 0.022)。结论:POAF与ICU-LOS时间延长、白种人、术中积液高有关。新发POAF与危重患者心脏骤停和死亡风险增加相关。
Postoperative atrial fibrillation in emergent non-cardiac surgery: Risk factors and outcomes from a ten-year intensive-care unit retrospective study.
Background: Atrial fibrillation (AF) represents a common arrhythmia with significant implications and may occur pre-, intra-, or postoperatively (POAF). After cardiac surgery POAF occurs in approximately 30% of patients, while non-cardiac/non-thoracic surgery has a reported incidence between 0.4% to 15%, with new onset POAF occurring at a rate of 0.4% to 3%. While AF has been extensively studied, it has not been well described in emergent non-cardiac surgery associated with increased surgical stress in an intensive care unit setting (ICU).
Aim: To investigate the incidence/predictors of POAF in emergent non-cardiac surgery and its associations with postoperative outcomes in the ICU.
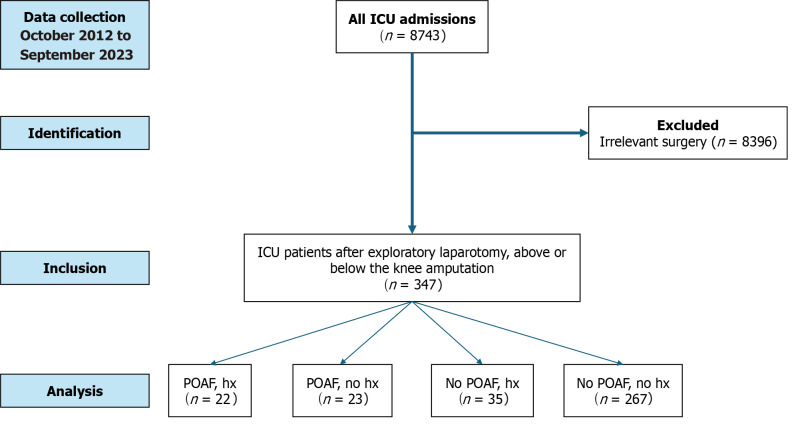
Methods: This retrospective study included patients ≥ 18 years who underwent exploratory laparotomy or lower extremity amputation between October 2012 and September 2023 and were admitted in the ICU. Data of interest included occurrence of POAF, demographic characteristics, comorbidities, laboratory values, administered fluids, medications, and postoperative outcomes. Statistical analyses consisted of identifying predictors of POAF and associations of POAF with outcomes of interest.
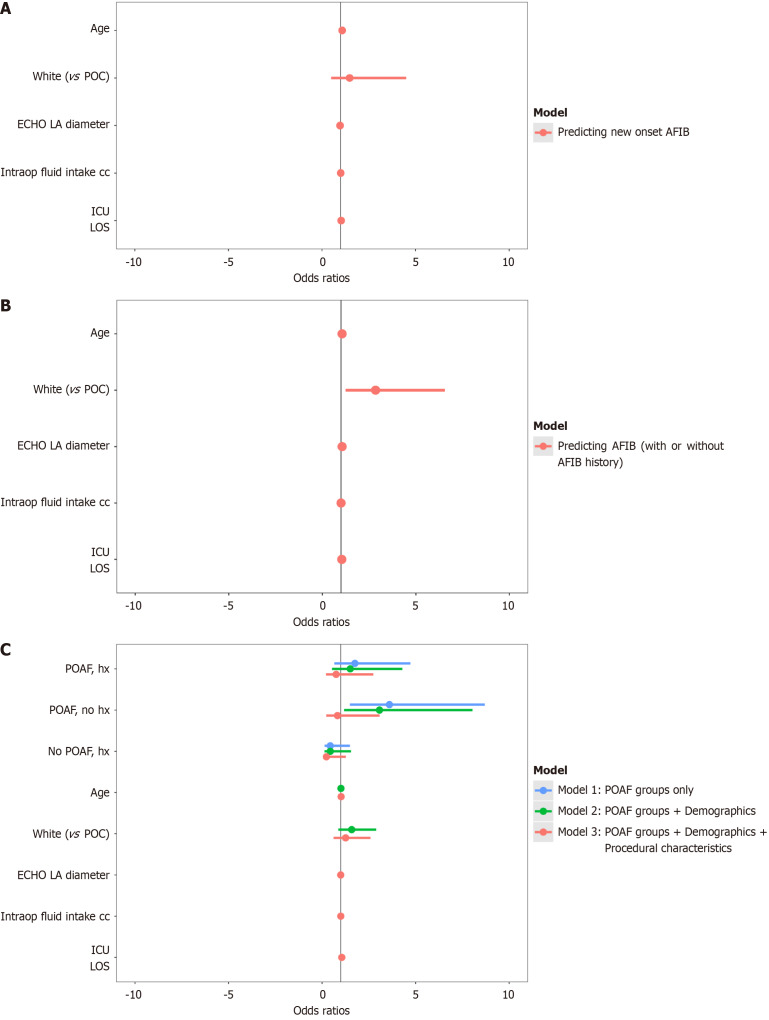
Results: A total of 347 ICU patients were included, 16.4% had a history of AF, 13.0% developed POAF, and 7.9% developed new-onset POAF. Patients with new-onset POAF were older (79.6 ± 9.1 vs 68.1 ± 14.8 years, < 0.001), of white race (47.8% vs 28.8, P < 0.001), hypertensive (87.0% vs 71.2%, P = 0.011), had longer ICU length of stay (ICU-LOS) (13.4 vs 6.7 days, P = 0.042), higher mortality (43.5% vs 17.6%, P = 0.016) and higher rate of cardiac arrest (34.8% vs 14.6%, P = 0.005) compared to patients without new-onset POAF. Multivariable analysis revealed increased POAF risk with advanced age (OR = 1.06; 95%CI: 1.02-1.10, P = 0.005), white race (OR = 2.85; 95%CI: 1.26-6.76, P = 0.014), high intraoperative fluid (OR > 1; 95%CI: 1.00-1.00, P = 0.018), and longer ICU-LOS (OR = 1.04; 95%CI: 1.00-1.08, P = 0.023). After adjusting for demographics, new onset POAF significantly predicted mortality (OR = 3.07; 95%CI: 1.14-8.01, P = 0.022).
Conclusion: POAF was associated with prolonged ICU-LOS, white race, and high intraoperative fluid. New-onset POAF was associated with increased risk of cardiac arrest and death in critically ill patients.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


