{"title":"脓毒症筛查工具、降钙素原和c反应蛋白在不明原因医院发烧中的诊断价值。","authors":"Shashikant Saini, Sapna Pahil, Ritin Mohindra, Naresh Sachdeva, Navneet Sharma, Ashok K Pannu","doi":"10.5492/wjccm.v14.i3.106496","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nosocomial fever of unknown origin (nFUO) is a frequent and challenging diagnostic entity, encompassing diverse infectious and non-infectious etiologies. Timely identification is crucial, yet evidence on the diagnostic accuracy of commonly employed sepsis screening tools and biomarkers remains sparse. We hypothesized that these tools and biomarkers measured at fever onset could distinguish infectious from non-infectious causes of nFUO in critically ill adults.</p><p><strong>Aim: </strong>To evaluate the diagnostic utility of sepsis tools and biomarkers in identifying infectious causes of nFUO.</p><p><strong>Methods: </strong>This prospective observational study included patients admitted to the Acute Care Emergency Medicine Unit, Postgraduate Institute of Medical Education and Research, Chandigarh, India (July 2023 to December 2024). nFUO was defined by Durack and Street criteria. Diagnostic performance of sepsis screening tools (systemic inflammatory response syndrome, Sequential Organ Failure Assessment, quick Sequential Organ Failure Assessment, National Early Warning Score, and Modified Early Warning Score) and biomarkers [procalcitonin (PCT), C-reactive protein (CRP)] at fever onset was assessed using receiver operating characteristic curve analysis.</p><p><strong>Results: </strong>Of 80 cases (mean age 42.9 ± 16.5 years; 80% male), 42.5% had infectious causes, 38.7% non-infectious, and 18.8% remained undiagnosed. Pneumonia (26.2%) and bloodstream infections (11.2%) were the most common infectious etiologies, while central fever and thrombophlebitis (each 7.5%) were predominant among non-infectious causes. Sepsis tools showed poor diagnostic accuracy, with area under the receiver operating characteristic curve (AUC) values close to 0.5. PCT demonstrated modest performance (AUC = 0.61; optimal cut-off: 0.85 μg/L), while CRP was paradoxically higher in non-infectious cases (AUC = 0.45). Overall mortality was 20% and was highest among undiagnosed patients (33.3%). Fever duration and hospitalization length were significantly greater in infectious cases.</p><p><strong>Conclusion: </strong>Sepsis tools, PCT, and CRP have limited utility in identifying infectious causes of nFUO in critically ill adults and should not solely guide initial decision-making.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"14 3","pages":"106496"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12305121/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic utility of sepsis screening tools, procalcitonin, and C-reactive protein in nosocomial fever of unknown origin.\",\"authors\":\"Shashikant Saini, Sapna Pahil, Ritin Mohindra, Naresh Sachdeva, Navneet Sharma, Ashok K Pannu\",\"doi\":\"10.5492/wjccm.v14.i3.106496\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Nosocomial fever of unknown origin (nFUO) is a frequent and challenging diagnostic entity, encompassing diverse infectious and non-infectious etiologies. Timely identification is crucial, yet evidence on the diagnostic accuracy of commonly employed sepsis screening tools and biomarkers remains sparse. We hypothesized that these tools and biomarkers measured at fever onset could distinguish infectious from non-infectious causes of nFUO in critically ill adults.</p><p><strong>Aim: </strong>To evaluate the diagnostic utility of sepsis tools and biomarkers in identifying infectious causes of nFUO.</p><p><strong>Methods: </strong>This prospective observational study included patients admitted to the Acute Care Emergency Medicine Unit, Postgraduate Institute of Medical Education and Research, Chandigarh, India (July 2023 to December 2024). nFUO was defined by Durack and Street criteria. Diagnostic performance of sepsis screening tools (systemic inflammatory response syndrome, Sequential Organ Failure Assessment, quick Sequential Organ Failure Assessment, National Early Warning Score, and Modified Early Warning Score) and biomarkers [procalcitonin (PCT), C-reactive protein (CRP)] at fever onset was assessed using receiver operating characteristic curve analysis.</p><p><strong>Results: </strong>Of 80 cases (mean age 42.9 ± 16.5 years; 80% male), 42.5% had infectious causes, 38.7% non-infectious, and 18.8% remained undiagnosed. Pneumonia (26.2%) and bloodstream infections (11.2%) were the most common infectious etiologies, while central fever and thrombophlebitis (each 7.5%) were predominant among non-infectious causes. Sepsis tools showed poor diagnostic accuracy, with area under the receiver operating characteristic curve (AUC) values close to 0.5. PCT demonstrated modest performance (AUC = 0.61; optimal cut-off: 0.85 μg/L), while CRP was paradoxically higher in non-infectious cases (AUC = 0.45). Overall mortality was 20% and was highest among undiagnosed patients (33.3%). Fever duration and hospitalization length were significantly greater in infectious cases.</p><p><strong>Conclusion: </strong>Sepsis tools, PCT, and CRP have limited utility in identifying infectious causes of nFUO in critically ill adults and should not solely guide initial decision-making.</p>\",\"PeriodicalId\":66959,\"journal\":{\"name\":\"世界危重病急救学杂志(英文版)\",\"volume\":\"14 3\",\"pages\":\"106496\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12305121/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"世界危重病急救学杂志(英文版)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5492/wjccm.v14.i3.106496\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5492/wjccm.v14.i3.106496","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Diagnostic utility of sepsis screening tools, procalcitonin, and C-reactive protein in nosocomial fever of unknown origin.
Background: Nosocomial fever of unknown origin (nFUO) is a frequent and challenging diagnostic entity, encompassing diverse infectious and non-infectious etiologies. Timely identification is crucial, yet evidence on the diagnostic accuracy of commonly employed sepsis screening tools and biomarkers remains sparse. We hypothesized that these tools and biomarkers measured at fever onset could distinguish infectious from non-infectious causes of nFUO in critically ill adults.
Aim: To evaluate the diagnostic utility of sepsis tools and biomarkers in identifying infectious causes of nFUO.
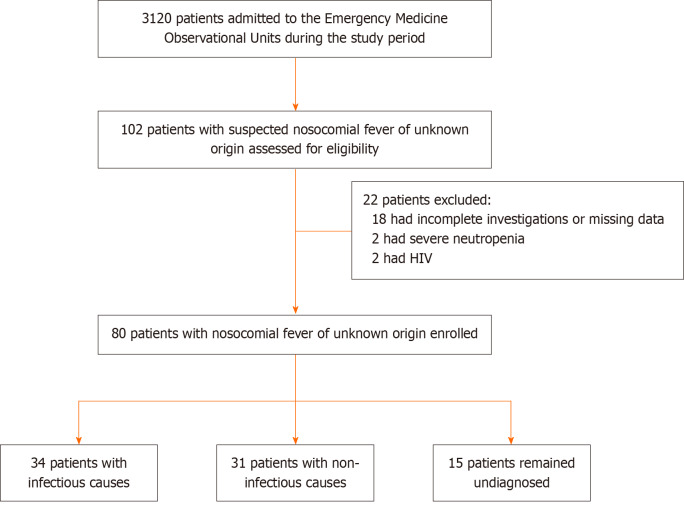
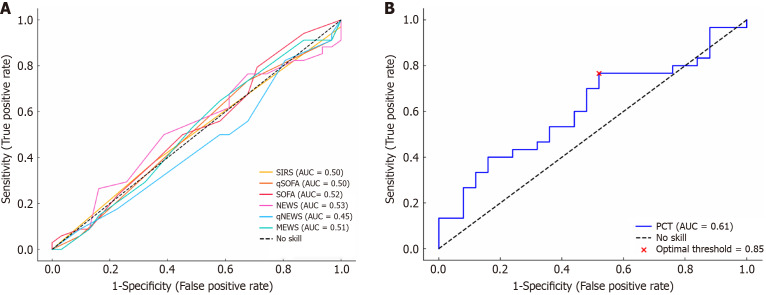
Methods: This prospective observational study included patients admitted to the Acute Care Emergency Medicine Unit, Postgraduate Institute of Medical Education and Research, Chandigarh, India (July 2023 to December 2024). nFUO was defined by Durack and Street criteria. Diagnostic performance of sepsis screening tools (systemic inflammatory response syndrome, Sequential Organ Failure Assessment, quick Sequential Organ Failure Assessment, National Early Warning Score, and Modified Early Warning Score) and biomarkers [procalcitonin (PCT), C-reactive protein (CRP)] at fever onset was assessed using receiver operating characteristic curve analysis.
Results: Of 80 cases (mean age 42.9 ± 16.5 years; 80% male), 42.5% had infectious causes, 38.7% non-infectious, and 18.8% remained undiagnosed. Pneumonia (26.2%) and bloodstream infections (11.2%) were the most common infectious etiologies, while central fever and thrombophlebitis (each 7.5%) were predominant among non-infectious causes. Sepsis tools showed poor diagnostic accuracy, with area under the receiver operating characteristic curve (AUC) values close to 0.5. PCT demonstrated modest performance (AUC = 0.61; optimal cut-off: 0.85 μg/L), while CRP was paradoxically higher in non-infectious cases (AUC = 0.45). Overall mortality was 20% and was highest among undiagnosed patients (33.3%). Fever duration and hospitalization length were significantly greater in infectious cases.
Conclusion: Sepsis tools, PCT, and CRP have limited utility in identifying infectious causes of nFUO in critically ill adults and should not solely guide initial decision-making.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


