Jacqueline Maree Williamson, Gillian Whalley, Simon Thornley, James Marangou, Peter Morris, Joshua R Francis, Vicki Wade, Bo Remenyi
{"title":"急性风湿热诊断对风湿性心脏病严重程度的影响。","authors":"Jacqueline Maree Williamson, Gillian Whalley, Simon Thornley, James Marangou, Peter Morris, Joshua R Francis, Vicki Wade, Bo Remenyi","doi":"10.5334/gh.1454","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute rheumatic fever (ARF) is the precursor to rheumatic heart disease (RHD) following Group A Streptococcal infection. However, many diagnoses of RHD are made in the absence of ARF history. We compared RHD severity between those with and those without a documented history of ARF.</p><p><strong>Methods: </strong>A retrospective audit of echocardiographic images determined RHD stage at diagnosis and at follow-up based on the 2023 WHF guidelines for the diagnosis of RHD.Individuals aged ≤ 20 years from the Top End of the Northern Territory (NT) of Australia with RHD diagnosis between January 2012 and December 2021 were included.Primary outcome was RHD stage at the time of diagnosis. Secondary outcomes were RHD stage progression or regression. Those with ARF and those with no ARF (noARF) were compared.</p><p><strong>Results: </strong>Study population (<i>n</i>) of 292 individuals with mean age 11.9 ± 3.8 years. At baseline, the ARF group had more Stage A RHD (28.6% versus 12.0%), while the noARF group had more Stage B (50.0% versus 38.0%), <i>p</i> = 0.009. There was no difference in advanced RHD (Stage C and D combined) between the groups (<i>p</i> = 0.440). Follow-up (median 46 months, IQR: 27-71 months) sample size was 230. Regression of RHD was greater in the ARF group (46% versus 28%, <i>p</i> = 0.014). No difference was found in stage progression (including to surgery), with 21% (32/156) in the ARF group and 15% (11/74) in the noARF group (<i>p</i> = 0.367).</p><p><strong>Conclusions: </strong>Individuals at all stages of RHD severity were detected amongst those with and without an accompanying diagnosis of ARF. Individuals with first RHD diagnosis accompanied by ARF were more likely to regress. These findings support echocardiographic screening in high-risk populations to detect early RHD that can be treated with secondary antibiotic prophylaxis. Further research is required to understand the reason for differences between the ARF and noARF groups.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"20 1","pages":"72"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396188/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of Acute Rheumatic Fever Diagnosis on Rheumatic Heart Disease Severity.\",\"authors\":\"Jacqueline Maree Williamson, Gillian Whalley, Simon Thornley, James Marangou, Peter Morris, Joshua R Francis, Vicki Wade, Bo Remenyi\",\"doi\":\"10.5334/gh.1454\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute rheumatic fever (ARF) is the precursor to rheumatic heart disease (RHD) following Group A Streptococcal infection. However, many diagnoses of RHD are made in the absence of ARF history. We compared RHD severity between those with and those without a documented history of ARF.</p><p><strong>Methods: </strong>A retrospective audit of echocardiographic images determined RHD stage at diagnosis and at follow-up based on the 2023 WHF guidelines for the diagnosis of RHD.Individuals aged ≤ 20 years from the Top End of the Northern Territory (NT) of Australia with RHD diagnosis between January 2012 and December 2021 were included.Primary outcome was RHD stage at the time of diagnosis. Secondary outcomes were RHD stage progression or regression. Those with ARF and those with no ARF (noARF) were compared.</p><p><strong>Results: </strong>Study population (<i>n</i>) of 292 individuals with mean age 11.9 ± 3.8 years. At baseline, the ARF group had more Stage A RHD (28.6% versus 12.0%), while the noARF group had more Stage B (50.0% versus 38.0%), <i>p</i> = 0.009. There was no difference in advanced RHD (Stage C and D combined) between the groups (<i>p</i> = 0.440). Follow-up (median 46 months, IQR: 27-71 months) sample size was 230. Regression of RHD was greater in the ARF group (46% versus 28%, <i>p</i> = 0.014). No difference was found in stage progression (including to surgery), with 21% (32/156) in the ARF group and 15% (11/74) in the noARF group (<i>p</i> = 0.367).</p><p><strong>Conclusions: </strong>Individuals at all stages of RHD severity were detected amongst those with and without an accompanying diagnosis of ARF. Individuals with first RHD diagnosis accompanied by ARF were more likely to regress. These findings support echocardiographic screening in high-risk populations to detect early RHD that can be treated with secondary antibiotic prophylaxis. Further research is required to understand the reason for differences between the ARF and noARF groups.</p>\",\"PeriodicalId\":56018,\"journal\":{\"name\":\"Global Heart\",\"volume\":\"20 1\",\"pages\":\"72\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396188/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global Heart\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5334/gh.1454\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1454","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The Impact of Acute Rheumatic Fever Diagnosis on Rheumatic Heart Disease Severity.
Background: Acute rheumatic fever (ARF) is the precursor to rheumatic heart disease (RHD) following Group A Streptococcal infection. However, many diagnoses of RHD are made in the absence of ARF history. We compared RHD severity between those with and those without a documented history of ARF.
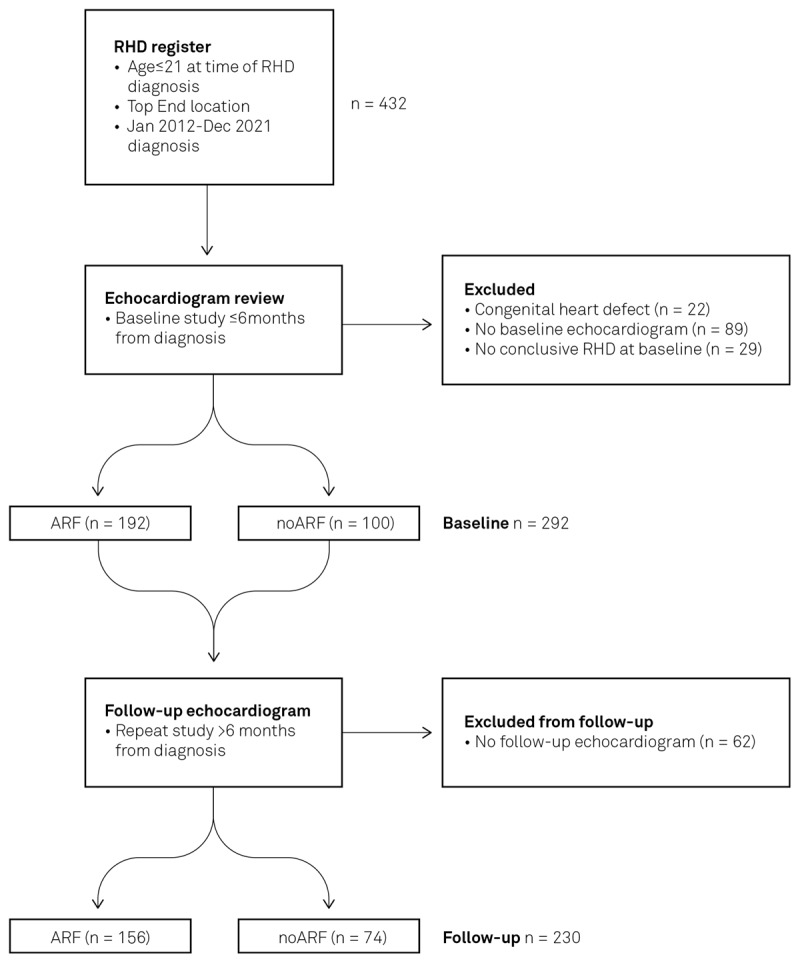
Methods: A retrospective audit of echocardiographic images determined RHD stage at diagnosis and at follow-up based on the 2023 WHF guidelines for the diagnosis of RHD.Individuals aged ≤ 20 years from the Top End of the Northern Territory (NT) of Australia with RHD diagnosis between January 2012 and December 2021 were included.Primary outcome was RHD stage at the time of diagnosis. Secondary outcomes were RHD stage progression or regression. Those with ARF and those with no ARF (noARF) were compared.
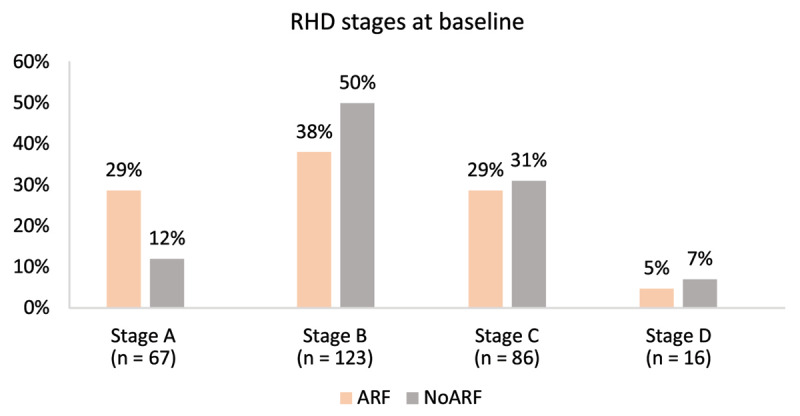
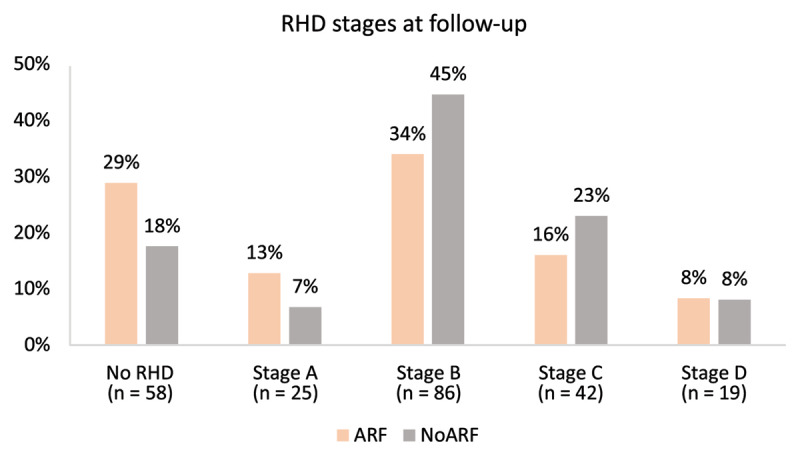
Results: Study population (n) of 292 individuals with mean age 11.9 ± 3.8 years. At baseline, the ARF group had more Stage A RHD (28.6% versus 12.0%), while the noARF group had more Stage B (50.0% versus 38.0%), p = 0.009. There was no difference in advanced RHD (Stage C and D combined) between the groups (p = 0.440). Follow-up (median 46 months, IQR: 27-71 months) sample size was 230. Regression of RHD was greater in the ARF group (46% versus 28%, p = 0.014). No difference was found in stage progression (including to surgery), with 21% (32/156) in the ARF group and 15% (11/74) in the noARF group (p = 0.367).
Conclusions: Individuals at all stages of RHD severity were detected amongst those with and without an accompanying diagnosis of ARF. Individuals with first RHD diagnosis accompanied by ARF were more likely to regress. These findings support echocardiographic screening in high-risk populations to detect early RHD that can be treated with secondary antibiotic prophylaxis. Further research is required to understand the reason for differences between the ARF and noARF groups.
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


