{"title":"肺腺癌中双EGFR L858R和KRAS G12A突变:罕见病例报告和文献复习。","authors":"Gang Wei, Jun Tang, Huaiwen Wang, Dongdong Zhang","doi":"10.2147/PGPM.S531038","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>KRAS mutations are typically mutually exclusive in non-small cell lung cancer (NSCLC), with the G12C mutation being the most common subtype. The coexistence of KRAS and EGFR mutations is exceedingly rare and is typically emerges as a secondary event following acquired resistance to EGFR-targeted therapies. We presented a case of a newly diagnosed NSCLC patient harboring concurrent EGFR L858R and KRAS G12A mutations.</p><p><strong>Case presentation: </strong>A 64-year-old male with a 30-pack-year smoking history presented with a 3-month history of progressive shortness of breath and chest tightness. Contrast-enhanced chest CT revealed a 5 cm spiculated mass in the right upper lobe, abutting the mediastinum, along with bronchial obstruction, right middle lobe atelectasis, and pleural effusion. A CT-guided transthoracic needle biopsy confirmed lung adenocarcinoma. Next-generation sequencing (NGS) identified a c.2573T>G (p.L858R) mutation in exon 21 of the EGFR gene and a c.35G>C (p.G12A) mutation in exon 2 of the KRAS gene. The patient started first-line therapy with osimertinib combined with pemetrexed/nedaplatin, resulting in a transient partial response, significant resolution of pleural effusion, and partial regression of the primary tumor. However, disease progression occurred within 6 months, marked by the appearance of a new cerebellar metastasis, confirmed by MRI. The patient continued osimertinib maintenance therapy and underwent stereotactic radiotherapy for the brain lesion. Despite initial stabilization, pulmonary progression was observed 11 months after the start of treatment. Due to declining performance status and personal preferences, the patient declined further treatment and was lost to follow-up.</p><p><strong>Conclusion: </strong>We report a rare case of treatment-naïve lung adenocarcinoma harboring concurrent KRAS G12A and EGFR L858R mutations. The patient achieved only transient disease control following treatment with a third-generation EGFR TKI combined with chemoradiotherapy. Further research to explore optimal therapeutic strategies for such complex molecular profiles is needed.</p>","PeriodicalId":56015,"journal":{"name":"Pharmacogenomics & Personalized Medicine","volume":"18 ","pages":"189-196"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12380001/pdf/","citationCount":"0","resultStr":"{\"title\":\"Dual EGFR L858R and KRAS G12A Mutations in Lung Adenocarcinoma: A Rare Case Report and Literature Review.\",\"authors\":\"Gang Wei, Jun Tang, Huaiwen Wang, Dongdong Zhang\",\"doi\":\"10.2147/PGPM.S531038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>KRAS mutations are typically mutually exclusive in non-small cell lung cancer (NSCLC), with the G12C mutation being the most common subtype. The coexistence of KRAS and EGFR mutations is exceedingly rare and is typically emerges as a secondary event following acquired resistance to EGFR-targeted therapies. We presented a case of a newly diagnosed NSCLC patient harboring concurrent EGFR L858R and KRAS G12A mutations.</p><p><strong>Case presentation: </strong>A 64-year-old male with a 30-pack-year smoking history presented with a 3-month history of progressive shortness of breath and chest tightness. Contrast-enhanced chest CT revealed a 5 cm spiculated mass in the right upper lobe, abutting the mediastinum, along with bronchial obstruction, right middle lobe atelectasis, and pleural effusion. A CT-guided transthoracic needle biopsy confirmed lung adenocarcinoma. Next-generation sequencing (NGS) identified a c.2573T>G (p.L858R) mutation in exon 21 of the EGFR gene and a c.35G>C (p.G12A) mutation in exon 2 of the KRAS gene. The patient started first-line therapy with osimertinib combined with pemetrexed/nedaplatin, resulting in a transient partial response, significant resolution of pleural effusion, and partial regression of the primary tumor. However, disease progression occurred within 6 months, marked by the appearance of a new cerebellar metastasis, confirmed by MRI. The patient continued osimertinib maintenance therapy and underwent stereotactic radiotherapy for the brain lesion. Despite initial stabilization, pulmonary progression was observed 11 months after the start of treatment. Due to declining performance status and personal preferences, the patient declined further treatment and was lost to follow-up.</p><p><strong>Conclusion: </strong>We report a rare case of treatment-naïve lung adenocarcinoma harboring concurrent KRAS G12A and EGFR L858R mutations. The patient achieved only transient disease control following treatment with a third-generation EGFR TKI combined with chemoradiotherapy. Further research to explore optimal therapeutic strategies for such complex molecular profiles is needed.</p>\",\"PeriodicalId\":56015,\"journal\":{\"name\":\"Pharmacogenomics & Personalized Medicine\",\"volume\":\"18 \",\"pages\":\"189-196\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12380001/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pharmacogenomics & Personalized Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/PGPM.S531038\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacogenomics & Personalized Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/PGPM.S531038","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Dual EGFR L858R and KRAS G12A Mutations in Lung Adenocarcinoma: A Rare Case Report and Literature Review.
Background: KRAS mutations are typically mutually exclusive in non-small cell lung cancer (NSCLC), with the G12C mutation being the most common subtype. The coexistence of KRAS and EGFR mutations is exceedingly rare and is typically emerges as a secondary event following acquired resistance to EGFR-targeted therapies. We presented a case of a newly diagnosed NSCLC patient harboring concurrent EGFR L858R and KRAS G12A mutations.
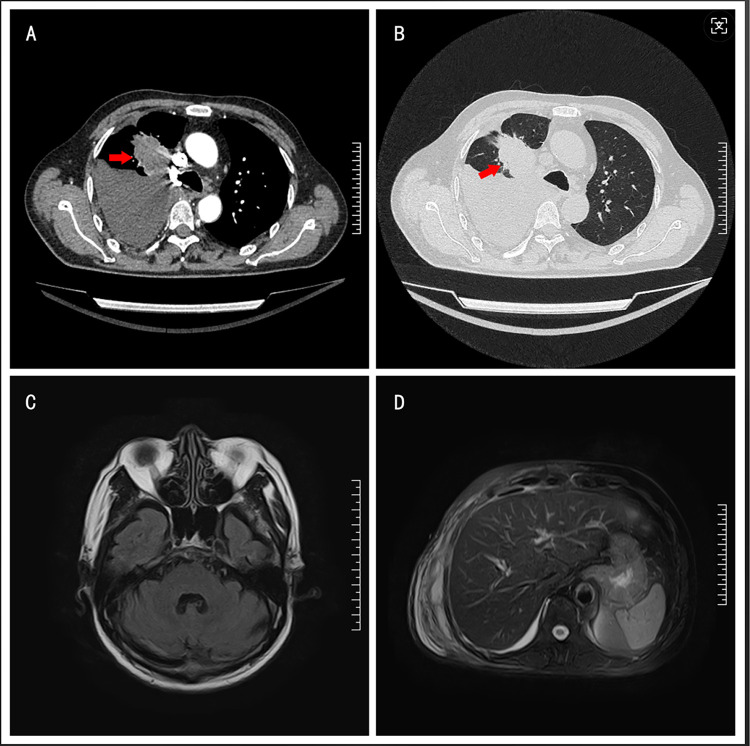
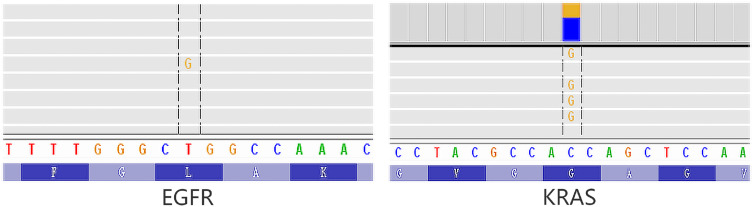
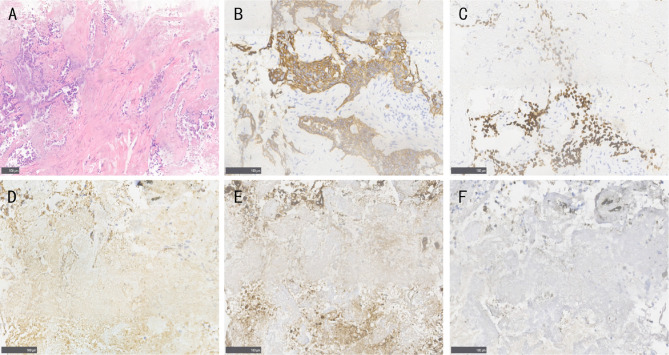
Case presentation: A 64-year-old male with a 30-pack-year smoking history presented with a 3-month history of progressive shortness of breath and chest tightness. Contrast-enhanced chest CT revealed a 5 cm spiculated mass in the right upper lobe, abutting the mediastinum, along with bronchial obstruction, right middle lobe atelectasis, and pleural effusion. A CT-guided transthoracic needle biopsy confirmed lung adenocarcinoma. Next-generation sequencing (NGS) identified a c.2573T>G (p.L858R) mutation in exon 21 of the EGFR gene and a c.35G>C (p.G12A) mutation in exon 2 of the KRAS gene. The patient started first-line therapy with osimertinib combined with pemetrexed/nedaplatin, resulting in a transient partial response, significant resolution of pleural effusion, and partial regression of the primary tumor. However, disease progression occurred within 6 months, marked by the appearance of a new cerebellar metastasis, confirmed by MRI. The patient continued osimertinib maintenance therapy and underwent stereotactic radiotherapy for the brain lesion. Despite initial stabilization, pulmonary progression was observed 11 months after the start of treatment. Due to declining performance status and personal preferences, the patient declined further treatment and was lost to follow-up.
Conclusion: We report a rare case of treatment-naïve lung adenocarcinoma harboring concurrent KRAS G12A and EGFR L858R mutations. The patient achieved only transient disease control following treatment with a third-generation EGFR TKI combined with chemoradiotherapy. Further research to explore optimal therapeutic strategies for such complex molecular profiles is needed.
期刊介绍:
Pharmacogenomics and Personalized Medicine is an international, peer-reviewed, open-access journal characterizing the influence of genotype on pharmacology leading to the development of personalized treatment programs and individualized drug selection for improved safety, efficacy and sustainability.
In particular, emphasis will be given to:
Genomic and proteomic profiling
Genetics and drug metabolism
Targeted drug identification and discovery
Optimizing drug selection & dosage based on patient''s genetic profile
Drug related morbidity & mortality intervention
Advanced disease screening and targeted therapeutic intervention
Genetic based vaccine development
Patient satisfaction and preference
Health economic evaluations
Practical and organizational issues in the development and implementation of personalized medicine programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


