{"title":"基于临床和CT特征的模型的开发和验证:预测非小细胞肺癌血管浸润的多变量分析。","authors":"Jieling Zhu, Fengjuan Tian, Zongyu Xie, Hengfeng Shi, Ting Yang, Xiaoyu Han, Cheng Yan, Fuquan Wei, Jian Wang","doi":"10.21037/qims-24-1886","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lymphovascular invasion (LVI) is a high-risk pathological marker for the evaluation of metastasis and prognosis of non-small cell lung cancer (NSCLC). Preoperative computed tomography (CT) prediction of vascular invasion in NSCLC is essential for clinical identification of high-risk patients and development of treatment strategies. This study aimed to develop and validate a model for predicting LVI in NSCLC based on clinical and CT features.</p><p><strong>Methods: </strong>A total of 2,830 patients with NSCLC confirmed by pathology and with complete clinical data were retrospectively enrolled. Among them, 2,663 were negative cases and 167 were positive cases. CT imaging and pathological data of these patients from Tongde Hospital of Zhejiang Province (center 1) and Anqing Municipal Hospital (center 2), from January 2015 to December 2023, were randomly divided into a training set and a validation set in a ratio of 7:3. Additionally, 275 patients from Taizhou Municipal Hospital (center 3) were assigned to the external validation set, including 242 negative cases and 33 positive cases. After screening for potential risk factors by univariate analysis, the selected risk factors were included in the multivariate binary logistic regression model to determine the independent risk factors of LVI in NSCLC to construct a prediction model and draw a nomogram, and the receiver operating characteristic (ROC) curve, calibration curve, and clinical impact curve (CIC) were used to evaluate the predictive power, discrimination, and clinical benefit of the model.</p><p><strong>Results: </strong>A total of 2,830 patients with NSCLC were included, including 1,190 (42.1%) males and 1,640 (57.9%) females, with a mean age of 61.15±10.83 years. Independent risk factors for LVI of NSCLC included the history of smoking, the history of diabetes mellitus, laboratory tumor indices, mixed ground-glass nodule (mGGN) consolidation/tumor ratio (CTR), and vacuole signs. The area under the curve (AUC), accuracy, sensitivity, and specificity for the training set were 0.836 [95% confidence interval (CI): 0.806-0.867], 65.2%, 92.1%, and 63.5%; those for the validation set were 0.803 (95% CI: 0.755-0.852), 71.6%, 82.7%, and 70.9%; and those for the external validation set were 0.845 (95% CI: 0.775-0.916), 70.9%, 87.8%, and 68.6%, respectively.</p><p><strong>Conclusions: </strong>We developed and validated a model for predicting LVI in NSCLC based on clinical and CT image features. The model developed in this study has potential application value in predicting LVI in NSCLC. It provides a new, operable, and non-invasive technique for clinical identification of high-risk patients and may help clinical selection of appropriate treatment.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8515-8528"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397630/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development and validation of models based on clinical and CT features: multivariate analysis for predicting vascular invasion in non-small cell lung cancer.\",\"authors\":\"Jieling Zhu, Fengjuan Tian, Zongyu Xie, Hengfeng Shi, Ting Yang, Xiaoyu Han, Cheng Yan, Fuquan Wei, Jian Wang\",\"doi\":\"10.21037/qims-24-1886\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Lymphovascular invasion (LVI) is a high-risk pathological marker for the evaluation of metastasis and prognosis of non-small cell lung cancer (NSCLC). Preoperative computed tomography (CT) prediction of vascular invasion in NSCLC is essential for clinical identification of high-risk patients and development of treatment strategies. This study aimed to develop and validate a model for predicting LVI in NSCLC based on clinical and CT features.</p><p><strong>Methods: </strong>A total of 2,830 patients with NSCLC confirmed by pathology and with complete clinical data were retrospectively enrolled. Among them, 2,663 were negative cases and 167 were positive cases. CT imaging and pathological data of these patients from Tongde Hospital of Zhejiang Province (center 1) and Anqing Municipal Hospital (center 2), from January 2015 to December 2023, were randomly divided into a training set and a validation set in a ratio of 7:3. Additionally, 275 patients from Taizhou Municipal Hospital (center 3) were assigned to the external validation set, including 242 negative cases and 33 positive cases. After screening for potential risk factors by univariate analysis, the selected risk factors were included in the multivariate binary logistic regression model to determine the independent risk factors of LVI in NSCLC to construct a prediction model and draw a nomogram, and the receiver operating characteristic (ROC) curve, calibration curve, and clinical impact curve (CIC) were used to evaluate the predictive power, discrimination, and clinical benefit of the model.</p><p><strong>Results: </strong>A total of 2,830 patients with NSCLC were included, including 1,190 (42.1%) males and 1,640 (57.9%) females, with a mean age of 61.15±10.83 years. Independent risk factors for LVI of NSCLC included the history of smoking, the history of diabetes mellitus, laboratory tumor indices, mixed ground-glass nodule (mGGN) consolidation/tumor ratio (CTR), and vacuole signs. The area under the curve (AUC), accuracy, sensitivity, and specificity for the training set were 0.836 [95% confidence interval (CI): 0.806-0.867], 65.2%, 92.1%, and 63.5%; those for the validation set were 0.803 (95% CI: 0.755-0.852), 71.6%, 82.7%, and 70.9%; and those for the external validation set were 0.845 (95% CI: 0.775-0.916), 70.9%, 87.8%, and 68.6%, respectively.</p><p><strong>Conclusions: </strong>We developed and validated a model for predicting LVI in NSCLC based on clinical and CT image features. The model developed in this study has potential application value in predicting LVI in NSCLC. It provides a new, operable, and non-invasive technique for clinical identification of high-risk patients and may help clinical selection of appropriate treatment.</p>\",\"PeriodicalId\":54267,\"journal\":{\"name\":\"Quantitative Imaging in Medicine and Surgery\",\"volume\":\"15 9\",\"pages\":\"8515-8528\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397630/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quantitative Imaging in Medicine and Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/qims-24-1886\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-24-1886","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Development and validation of models based on clinical and CT features: multivariate analysis for predicting vascular invasion in non-small cell lung cancer.
Background: Lymphovascular invasion (LVI) is a high-risk pathological marker for the evaluation of metastasis and prognosis of non-small cell lung cancer (NSCLC). Preoperative computed tomography (CT) prediction of vascular invasion in NSCLC is essential for clinical identification of high-risk patients and development of treatment strategies. This study aimed to develop and validate a model for predicting LVI in NSCLC based on clinical and CT features.
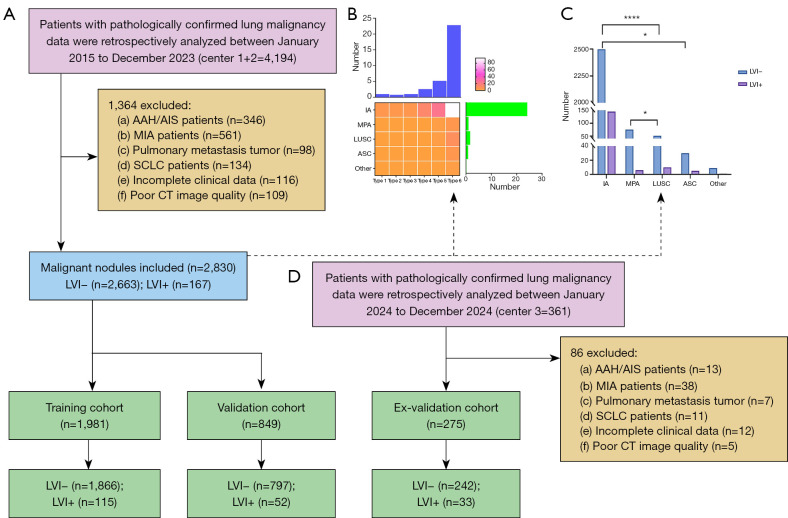
Methods: A total of 2,830 patients with NSCLC confirmed by pathology and with complete clinical data were retrospectively enrolled. Among them, 2,663 were negative cases and 167 were positive cases. CT imaging and pathological data of these patients from Tongde Hospital of Zhejiang Province (center 1) and Anqing Municipal Hospital (center 2), from January 2015 to December 2023, were randomly divided into a training set and a validation set in a ratio of 7:3. Additionally, 275 patients from Taizhou Municipal Hospital (center 3) were assigned to the external validation set, including 242 negative cases and 33 positive cases. After screening for potential risk factors by univariate analysis, the selected risk factors were included in the multivariate binary logistic regression model to determine the independent risk factors of LVI in NSCLC to construct a prediction model and draw a nomogram, and the receiver operating characteristic (ROC) curve, calibration curve, and clinical impact curve (CIC) were used to evaluate the predictive power, discrimination, and clinical benefit of the model.
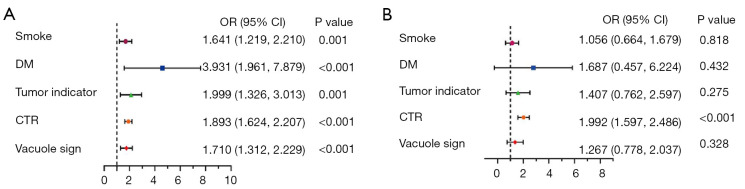
Results: A total of 2,830 patients with NSCLC were included, including 1,190 (42.1%) males and 1,640 (57.9%) females, with a mean age of 61.15±10.83 years. Independent risk factors for LVI of NSCLC included the history of smoking, the history of diabetes mellitus, laboratory tumor indices, mixed ground-glass nodule (mGGN) consolidation/tumor ratio (CTR), and vacuole signs. The area under the curve (AUC), accuracy, sensitivity, and specificity for the training set were 0.836 [95% confidence interval (CI): 0.806-0.867], 65.2%, 92.1%, and 63.5%; those for the validation set were 0.803 (95% CI: 0.755-0.852), 71.6%, 82.7%, and 70.9%; and those for the external validation set were 0.845 (95% CI: 0.775-0.916), 70.9%, 87.8%, and 68.6%, respectively.
Conclusions: We developed and validated a model for predicting LVI in NSCLC based on clinical and CT image features. The model developed in this study has potential application value in predicting LVI in NSCLC. It provides a new, operable, and non-invasive technique for clinical identification of high-risk patients and may help clinical selection of appropriate treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


