Jin Tang, Jianing Wang, Tao Li, Siyu Wang, Zhengping Liu, Xue Du, Xiaokun Wang, Wei Xie, Jinfeng Hu, Xugui Li
{"title":"经皮内镜后路腰椎椎间融合术及改良后路腰椎椎间融合术治疗腰椎退行性疾病的影像学指标及融合分析","authors":"Jin Tang, Jianing Wang, Tao Li, Siyu Wang, Zhengping Liu, Xue Du, Xiaokun Wang, Wei Xie, Jinfeng Hu, Xugui Li","doi":"10.21037/qims-24-2268","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although numerous studies have confirmed percutaneous endoscopic posterior lumbar interbody fusion (PE-PLIF) as a safe and effective minimally invasive technique for lumbar degenerative diseases (LDDs), existing research primarily focuses on clinical outcomes and involves limited imaging analysis. This study aimed to quantitatively compare PE-PLIF and modified posterior lumbar interbody fusion (MPLIF) through comprehensive radiographic evaluation and clinical outcomes.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 75 consecutive LDD patients who underwent surgical treatment at our institution between January 2018 and October 2023. The patients were divided into an observation group (PE-PLIF; 36 cases) and a control group (MPLIF; 39 cases) according to their surgical approach. The intervertebral space height (mm), segmental Cobb angle (°), bone graft area (mm<sup>2</sup>), and bone graft range were recorded and compared for each patient during the preoperative period, the first postoperative review, and the final follow-up. Additionally, the fusion rates, operative time, intraoperative blood loss (IBL), time to ambulation post-surgery, length of postoperative hospital stay, and complications were compared between the two groups at 3 and 6 months postoperatively.</p><p><strong>Results: </strong>Complete follow-up data showed significant postoperative improvement in both groups (all P<0.001). The PE-PLIF group showed better results, with the intervertebral height increasing from 11.59±2.04 to 14.67±1.62 mm (an improvement of 26.6%), whereas the MPLIF group increased from 10.67±1.25 to 12.64±2.58 mm (an improvement of 18.5%). At the final follow-up, a high recovery rate of 16.1% was maintained (13.53±1.26 <i>vs</i>. 10.74±4.53 mm, P<0.001). Cobb angle correction also demonstrated similar advantages. The PE-PLIF improved from 17.01°±10.84° to 20.65°±6.42° (21.4% correction), whereas the MPLIF improved from 16.05°±7.43° to 18.54°±5.13° (15.5% correction). The final alignment of PE-PLIF remained better (18.73°±8.95° to 17.52°±7.33°, P<0.001). The surgical results showed that the required bone graft volume for PE-PLIF decreased by 12.4% (478.70±97.50 and 546.67±101.39 mm<sup>2</sup>, P=0.004), and the average operation time was significantly longer than that of the MPLIF group (P<0.001). However, the IBL was significantly less than that in the MPLIF group (P<0.001). The postoperative bed rest time in the PE-PLIF group was significantly shorter than that in the MPLIF group (P<0.001). The postoperative hospital stay in the PE-PLIF group was significantly shorter than that in the MPLIF group (P<0.001). Both procedures were completed successfully with no major complications.</p><p><strong>Conclusions: </strong>PE-PLIF demonstrates superior efficacy over MPLIF in restoring intervertebral height and stability, with advantages including reduced blood loss, better endplate preservation, reliable fusion rates, and faster recovery. These findings suggest that PE-PLIF is a safer, more effective minimally invasive option for LDD treatment, and further validation is warranted.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8079-8095"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397665/pdf/","citationCount":"0","resultStr":"{\"title\":\"Imaging indicators and fusion analysis of percutaneous endoscopic posterior lumbar interbody fusion and modified posterior lumbar interbody fusion for the treatment of lumbar degenerative diseases.\",\"authors\":\"Jin Tang, Jianing Wang, Tao Li, Siyu Wang, Zhengping Liu, Xue Du, Xiaokun Wang, Wei Xie, Jinfeng Hu, Xugui Li\",\"doi\":\"10.21037/qims-24-2268\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Although numerous studies have confirmed percutaneous endoscopic posterior lumbar interbody fusion (PE-PLIF) as a safe and effective minimally invasive technique for lumbar degenerative diseases (LDDs), existing research primarily focuses on clinical outcomes and involves limited imaging analysis. This study aimed to quantitatively compare PE-PLIF and modified posterior lumbar interbody fusion (MPLIF) through comprehensive radiographic evaluation and clinical outcomes.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 75 consecutive LDD patients who underwent surgical treatment at our institution between January 2018 and October 2023. The patients were divided into an observation group (PE-PLIF; 36 cases) and a control group (MPLIF; 39 cases) according to their surgical approach. The intervertebral space height (mm), segmental Cobb angle (°), bone graft area (mm<sup>2</sup>), and bone graft range were recorded and compared for each patient during the preoperative period, the first postoperative review, and the final follow-up. Additionally, the fusion rates, operative time, intraoperative blood loss (IBL), time to ambulation post-surgery, length of postoperative hospital stay, and complications were compared between the two groups at 3 and 6 months postoperatively.</p><p><strong>Results: </strong>Complete follow-up data showed significant postoperative improvement in both groups (all P<0.001). The PE-PLIF group showed better results, with the intervertebral height increasing from 11.59±2.04 to 14.67±1.62 mm (an improvement of 26.6%), whereas the MPLIF group increased from 10.67±1.25 to 12.64±2.58 mm (an improvement of 18.5%). At the final follow-up, a high recovery rate of 16.1% was maintained (13.53±1.26 <i>vs</i>. 10.74±4.53 mm, P<0.001). Cobb angle correction also demonstrated similar advantages. The PE-PLIF improved from 17.01°±10.84° to 20.65°±6.42° (21.4% correction), whereas the MPLIF improved from 16.05°±7.43° to 18.54°±5.13° (15.5% correction). The final alignment of PE-PLIF remained better (18.73°±8.95° to 17.52°±7.33°, P<0.001). The surgical results showed that the required bone graft volume for PE-PLIF decreased by 12.4% (478.70±97.50 and 546.67±101.39 mm<sup>2</sup>, P=0.004), and the average operation time was significantly longer than that of the MPLIF group (P<0.001). However, the IBL was significantly less than that in the MPLIF group (P<0.001). The postoperative bed rest time in the PE-PLIF group was significantly shorter than that in the MPLIF group (P<0.001). The postoperative hospital stay in the PE-PLIF group was significantly shorter than that in the MPLIF group (P<0.001). Both procedures were completed successfully with no major complications.</p><p><strong>Conclusions: </strong>PE-PLIF demonstrates superior efficacy over MPLIF in restoring intervertebral height and stability, with advantages including reduced blood loss, better endplate preservation, reliable fusion rates, and faster recovery. These findings suggest that PE-PLIF is a safer, more effective minimally invasive option for LDD treatment, and further validation is warranted.</p>\",\"PeriodicalId\":54267,\"journal\":{\"name\":\"Quantitative Imaging in Medicine and Surgery\",\"volume\":\"15 9\",\"pages\":\"8079-8095\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397665/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quantitative Imaging in Medicine and Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/qims-24-2268\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-24-2268","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Imaging indicators and fusion analysis of percutaneous endoscopic posterior lumbar interbody fusion and modified posterior lumbar interbody fusion for the treatment of lumbar degenerative diseases.
Background: Although numerous studies have confirmed percutaneous endoscopic posterior lumbar interbody fusion (PE-PLIF) as a safe and effective minimally invasive technique for lumbar degenerative diseases (LDDs), existing research primarily focuses on clinical outcomes and involves limited imaging analysis. This study aimed to quantitatively compare PE-PLIF and modified posterior lumbar interbody fusion (MPLIF) through comprehensive radiographic evaluation and clinical outcomes.
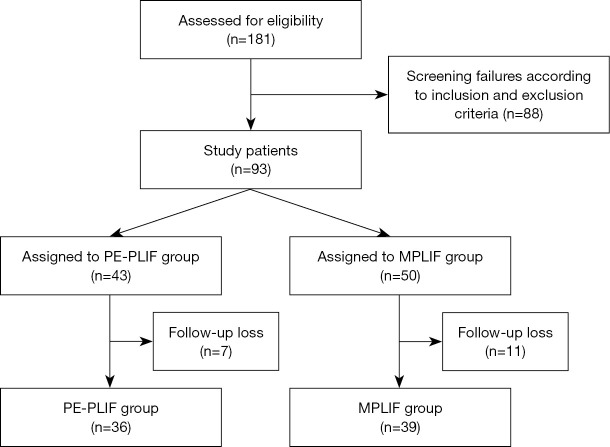
Methods: We conducted a retrospective analysis of 75 consecutive LDD patients who underwent surgical treatment at our institution between January 2018 and October 2023. The patients were divided into an observation group (PE-PLIF; 36 cases) and a control group (MPLIF; 39 cases) according to their surgical approach. The intervertebral space height (mm), segmental Cobb angle (°), bone graft area (mm2), and bone graft range were recorded and compared for each patient during the preoperative period, the first postoperative review, and the final follow-up. Additionally, the fusion rates, operative time, intraoperative blood loss (IBL), time to ambulation post-surgery, length of postoperative hospital stay, and complications were compared between the two groups at 3 and 6 months postoperatively.
Results: Complete follow-up data showed significant postoperative improvement in both groups (all P<0.001). The PE-PLIF group showed better results, with the intervertebral height increasing from 11.59±2.04 to 14.67±1.62 mm (an improvement of 26.6%), whereas the MPLIF group increased from 10.67±1.25 to 12.64±2.58 mm (an improvement of 18.5%). At the final follow-up, a high recovery rate of 16.1% was maintained (13.53±1.26 vs. 10.74±4.53 mm, P<0.001). Cobb angle correction also demonstrated similar advantages. The PE-PLIF improved from 17.01°±10.84° to 20.65°±6.42° (21.4% correction), whereas the MPLIF improved from 16.05°±7.43° to 18.54°±5.13° (15.5% correction). The final alignment of PE-PLIF remained better (18.73°±8.95° to 17.52°±7.33°, P<0.001). The surgical results showed that the required bone graft volume for PE-PLIF decreased by 12.4% (478.70±97.50 and 546.67±101.39 mm2, P=0.004), and the average operation time was significantly longer than that of the MPLIF group (P<0.001). However, the IBL was significantly less than that in the MPLIF group (P<0.001). The postoperative bed rest time in the PE-PLIF group was significantly shorter than that in the MPLIF group (P<0.001). The postoperative hospital stay in the PE-PLIF group was significantly shorter than that in the MPLIF group (P<0.001). Both procedures were completed successfully with no major complications.
Conclusions: PE-PLIF demonstrates superior efficacy over MPLIF in restoring intervertebral height and stability, with advantages including reduced blood loss, better endplate preservation, reliable fusion rates, and faster recovery. These findings suggest that PE-PLIF is a safer, more effective minimally invasive option for LDD treatment, and further validation is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


