{"title":"基于18F-FDG PET/CT的术前病变全糖溶解与淋巴血管侵袭的相关性及其对原发性胃癌的预测价值:一项横断面研究。","authors":"Xiu-Qing Xue, Xiao-Feng Li, Xun Shi, Yue-Tao Wang","doi":"10.21037/qims-2025-644","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lymphovascular invasion (LVI) is a critical factor in the lymphatic spread of tumor cells, and is closely associated with local recurrence and distant metastasis in gastric cancer. The study aimed to evaluate the correlation and predictive value of preoperative total lesion glycolysis (TLG) in patients with primary gastric cancer as measured by a combination of <sup>18</sup>F-labeled fluoro-2-deoxyglucose (<sup>18</sup>F-FDG) positron emission tomography (PET) and computed tomography (CT) for LVI.</p><p><strong>Methods: </strong>A retrospective analysis of the demographic and <sup>18</sup>F-FDG PET/CT data of 177 patients with gastric cancer diagnosed by postoperative pathology at The Third Affiliated Hospital of Soochow University between January 2014 and August 2021 was conducted. The cohort comprised 124 males and 53 females. The <sup>18</sup>F-FDG PET/CT data analyzed included the primary lesion location and size, lymph node metastasis (LNM) status, and metabolic parameters [i.e., the maximum standardized uptake value (SUVmax), mean standardized uptake value (SUVmean), metabolic tumor volume (MTV), and TLG]. The patients were categorized into LVI-positive (LVI+) and LVI-negative (LVI-) groups based on postoperative pathological findings. Differences in the clinical data between the two groups were analyzed. Univariate and multivariate logistic regression models were employed to assess the correlation between preoperative TLG and LVI. A generalized additive model (GAM) was applied for curve fitting, and receiver operating characteristic (ROC) curves were plotted to evaluate the predictive efficacy of preoperative TLG for LVI.</p><p><strong>Results: </strong>Among the 177 patients, 71 (40.1%) were LVI+, and 106 (59.9%) were LVI-. Significant differences were observed between the two groups in terms of the primary lesion size, LNM status, age, SUVmax, SUVmean, MTV, and TLG (all P<0.05 or P<0.001). A per standard deviation (SD) increase in TLG was associated with a 59.1% increased risk of LVI [odds ratio (OR) =1.591; 95% confidence interval (CI): 1.142-2.216; P=0.006]. After adjusting for confounders, TLG remained significantly associated with an increased risk of LVI (OR per SD: 1.428; 95% CI: 1.018-2.002; P=0.039). Treating TLG as a categorical variable produced consistent results (P for trend =0.014). In the clinical lymph node metastasis positive (cLNM+) subgroup, a TLG value ≥53.3 predicted LVI with a sensitivity of 81.4% (35/43), a specificity of 37.8% (14/37), and an accuracy of 61.3% (49/80). In the clinical lymph node metastasis negative (cLNM-) subgroup, a TLG value ≥41.9 predicted LVI with a sensitivity of 82.1% (23/28), a specificity of 53.6% (37/69), and an accuracy of 61.9% (60/97).</p><p><strong>Conclusions: </strong>Preoperative TLG exhibits a positive linear correlation with the risk of LVI in primary gastric cancer. TLG shows high sensitivity for predicting LVI, making it a valuable imaging biomarker for assessing LVI risk in gastric cancer, especially in cLNM- but LVI+ patients.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"7738-7748"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397669/pdf/","citationCount":"0","resultStr":"{\"title\":\"The correlation between preoperative total lesion glycolysis and lymphovascular invasion based on <sup>18</sup>F-FDG PET/CT and its predictive value in primary gastric cancer: a cross-sectional study.\",\"authors\":\"Xiu-Qing Xue, Xiao-Feng Li, Xun Shi, Yue-Tao Wang\",\"doi\":\"10.21037/qims-2025-644\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Lymphovascular invasion (LVI) is a critical factor in the lymphatic spread of tumor cells, and is closely associated with local recurrence and distant metastasis in gastric cancer. The study aimed to evaluate the correlation and predictive value of preoperative total lesion glycolysis (TLG) in patients with primary gastric cancer as measured by a combination of <sup>18</sup>F-labeled fluoro-2-deoxyglucose (<sup>18</sup>F-FDG) positron emission tomography (PET) and computed tomography (CT) for LVI.</p><p><strong>Methods: </strong>A retrospective analysis of the demographic and <sup>18</sup>F-FDG PET/CT data of 177 patients with gastric cancer diagnosed by postoperative pathology at The Third Affiliated Hospital of Soochow University between January 2014 and August 2021 was conducted. The cohort comprised 124 males and 53 females. The <sup>18</sup>F-FDG PET/CT data analyzed included the primary lesion location and size, lymph node metastasis (LNM) status, and metabolic parameters [i.e., the maximum standardized uptake value (SUVmax), mean standardized uptake value (SUVmean), metabolic tumor volume (MTV), and TLG]. The patients were categorized into LVI-positive (LVI+) and LVI-negative (LVI-) groups based on postoperative pathological findings. Differences in the clinical data between the two groups were analyzed. Univariate and multivariate logistic regression models were employed to assess the correlation between preoperative TLG and LVI. A generalized additive model (GAM) was applied for curve fitting, and receiver operating characteristic (ROC) curves were plotted to evaluate the predictive efficacy of preoperative TLG for LVI.</p><p><strong>Results: </strong>Among the 177 patients, 71 (40.1%) were LVI+, and 106 (59.9%) were LVI-. Significant differences were observed between the two groups in terms of the primary lesion size, LNM status, age, SUVmax, SUVmean, MTV, and TLG (all P<0.05 or P<0.001). A per standard deviation (SD) increase in TLG was associated with a 59.1% increased risk of LVI [odds ratio (OR) =1.591; 95% confidence interval (CI): 1.142-2.216; P=0.006]. After adjusting for confounders, TLG remained significantly associated with an increased risk of LVI (OR per SD: 1.428; 95% CI: 1.018-2.002; P=0.039). Treating TLG as a categorical variable produced consistent results (P for trend =0.014). In the clinical lymph node metastasis positive (cLNM+) subgroup, a TLG value ≥53.3 predicted LVI with a sensitivity of 81.4% (35/43), a specificity of 37.8% (14/37), and an accuracy of 61.3% (49/80). In the clinical lymph node metastasis negative (cLNM-) subgroup, a TLG value ≥41.9 predicted LVI with a sensitivity of 82.1% (23/28), a specificity of 53.6% (37/69), and an accuracy of 61.9% (60/97).</p><p><strong>Conclusions: </strong>Preoperative TLG exhibits a positive linear correlation with the risk of LVI in primary gastric cancer. TLG shows high sensitivity for predicting LVI, making it a valuable imaging biomarker for assessing LVI risk in gastric cancer, especially in cLNM- but LVI+ patients.</p>\",\"PeriodicalId\":54267,\"journal\":{\"name\":\"Quantitative Imaging in Medicine and Surgery\",\"volume\":\"15 9\",\"pages\":\"7738-7748\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397669/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quantitative Imaging in Medicine and Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/qims-2025-644\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-2025-644","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
The correlation between preoperative total lesion glycolysis and lymphovascular invasion based on 18F-FDG PET/CT and its predictive value in primary gastric cancer: a cross-sectional study.
Background: Lymphovascular invasion (LVI) is a critical factor in the lymphatic spread of tumor cells, and is closely associated with local recurrence and distant metastasis in gastric cancer. The study aimed to evaluate the correlation and predictive value of preoperative total lesion glycolysis (TLG) in patients with primary gastric cancer as measured by a combination of 18F-labeled fluoro-2-deoxyglucose (18F-FDG) positron emission tomography (PET) and computed tomography (CT) for LVI.
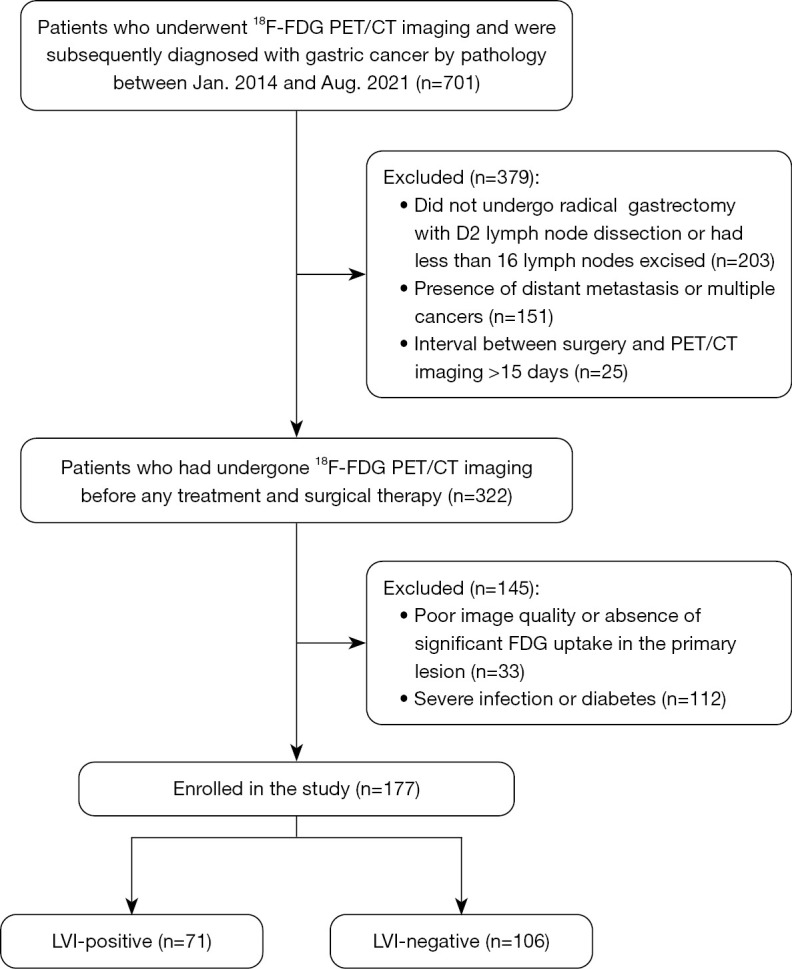
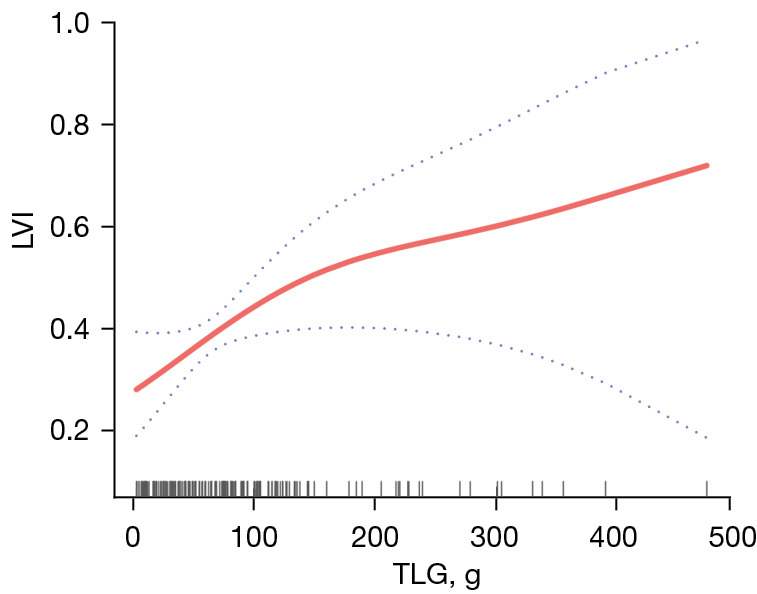
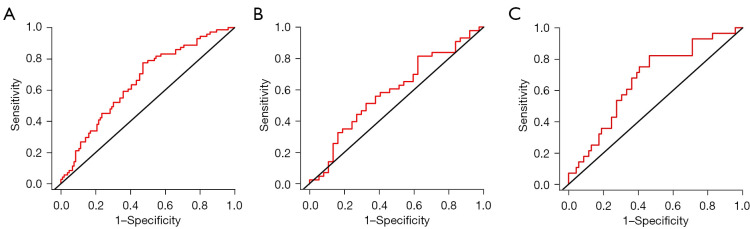
Methods: A retrospective analysis of the demographic and 18F-FDG PET/CT data of 177 patients with gastric cancer diagnosed by postoperative pathology at The Third Affiliated Hospital of Soochow University between January 2014 and August 2021 was conducted. The cohort comprised 124 males and 53 females. The 18F-FDG PET/CT data analyzed included the primary lesion location and size, lymph node metastasis (LNM) status, and metabolic parameters [i.e., the maximum standardized uptake value (SUVmax), mean standardized uptake value (SUVmean), metabolic tumor volume (MTV), and TLG]. The patients were categorized into LVI-positive (LVI+) and LVI-negative (LVI-) groups based on postoperative pathological findings. Differences in the clinical data between the two groups were analyzed. Univariate and multivariate logistic regression models were employed to assess the correlation between preoperative TLG and LVI. A generalized additive model (GAM) was applied for curve fitting, and receiver operating characteristic (ROC) curves were plotted to evaluate the predictive efficacy of preoperative TLG for LVI.
Results: Among the 177 patients, 71 (40.1%) were LVI+, and 106 (59.9%) were LVI-. Significant differences were observed between the two groups in terms of the primary lesion size, LNM status, age, SUVmax, SUVmean, MTV, and TLG (all P<0.05 or P<0.001). A per standard deviation (SD) increase in TLG was associated with a 59.1% increased risk of LVI [odds ratio (OR) =1.591; 95% confidence interval (CI): 1.142-2.216; P=0.006]. After adjusting for confounders, TLG remained significantly associated with an increased risk of LVI (OR per SD: 1.428; 95% CI: 1.018-2.002; P=0.039). Treating TLG as a categorical variable produced consistent results (P for trend =0.014). In the clinical lymph node metastasis positive (cLNM+) subgroup, a TLG value ≥53.3 predicted LVI with a sensitivity of 81.4% (35/43), a specificity of 37.8% (14/37), and an accuracy of 61.3% (49/80). In the clinical lymph node metastasis negative (cLNM-) subgroup, a TLG value ≥41.9 predicted LVI with a sensitivity of 82.1% (23/28), a specificity of 53.6% (37/69), and an accuracy of 61.9% (60/97).
Conclusions: Preoperative TLG exhibits a positive linear correlation with the risk of LVI in primary gastric cancer. TLG shows high sensitivity for predicting LVI, making it a valuable imaging biomarker for assessing LVI risk in gastric cancer, especially in cLNM- but LVI+ patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


