Rui Wang, Shuo Leng, Han Xu, Zhiming Tian, Shujuan Xu, Yi Zhang
{"title":"双容积重建技术在颅内动脉瘤栓塞后复发动脉瘤的检测与分型中的应用。","authors":"Rui Wang, Shuo Leng, Han Xu, Zhiming Tian, Shujuan Xu, Yi Zhang","doi":"10.21037/qims-2025-303","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accurate detection of recurrent intracranial aneurysms (ICAs) after embolization is critical for guiding clinical management and preventing re-rupture. Although two-dimensional digital subtraction angiography (2D-DSA) remains the gold standard, its invasive nature limits routine use. Non-invasive imaging modalities such as computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have limitations in detecting small or morphologically complex recurrent aneurysms. This study aimed to evaluate the diagnostic performance of dual-volume reconstruction technology (DVRT) in comparison to CTA and MRA for detecting recurrent ICA and to explore the correlation between aneurysm imaging characteristics and clinical outcomes.</p><p><strong>Methods: </strong>This retrospective study included 152 patients who underwent ICA embolization and subsequent follow-up imaging with CTA, MRA, and DVRT. All patients received standardized pre-procedural imaging (CTA, MRA, and DVRT) within 48 hours before intervention to document baseline aneurysm characteristics including size, morphology, and location. Postoperative surveillance was systematically performed using triple-modality imaging (CTA, MRA, and DVRT) at 3- and 12-month intervals to monitor treatment efficacy and detect potential recurrence. For the classification of recurrent aneurysms, post-embolization imaging attributes (size, morphology, location) were compared to pre-embolization baseline data to confirm recurrence. Multivariable logistic regression analysis was applied to pre-embolization characteristics to predict recurrence risk. Visualization techniques, including heatmaps and forest plots, were used to illustrate comparative detection performance.</p><p><strong>Results: </strong>DVRT demonstrated higher detection rates for recurrent aneurysms (94.4%, 17/18) compared to CTA (77.8%, 14/18) and MRA (50.0%, 9/18) (P<0.001), with notable performance for small aneurysms (<5 mm: 80.0% <i>vs.</i> 60.0% <i>vs.</i> 40.0%; P=0.317) and medium aneurysms (5-10 mm: 100.0% <i>vs.</i> 88.9% <i>vs.</i> 55.6%; P=0.012). Morphological analysis showed that DVRT had high detection rates for saccular (100.0% <i>vs.</i> 88.9% <i>vs.</i> 66.7%; P=0.039) and lobulated aneurysms (100.0% <i>vs.</i> 75.0% <i>vs.</i> 50.0%; P=0.250), while maintaining detection rates of 92.3% for anterior circulation (<i>vs.</i> 76.9% <i>vs.</i> 46.2%; P=0.008) and 100.0% for posterior circulation aneurysms (<i>vs.</i> 80.0% <i>vs.</i> 60.0%; P=0.200) compared to CTA and MRA, respectively. Multivariable analysis identified size >10 mm [odds ratio (OR) =2.51, 95% confidence interval (CI): 1.83-3.51, P=0.030], irregular morphology (OR =3.02, 95% CI: 2.15-4.43, P=0.003), and posterior location (OR =2.07, 95% CI: 1.43-2.91, P<0.001) as independent predictors of recurrence. Heatmap and forest plot analyses highlighted DVRT's improved diagnostic consistency and narrower CIs across different aneurysm subtypes.</p><p><strong>Conclusions: </strong>DVRT offers superior diagnostic accuracy in detecting recurrent ICA following embolization compared to CTA and MRA, particularly for small, irregularly shaped, and posterior circulation aneurysms. Its advanced imaging capabilities support early detection of recurrence, informed risk stratification, and optimized clinical management strategies. Integration of DVRT into routine postoperative surveillance may improve long-term outcomes for patients with ICA.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8008-8022"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397631/pdf/","citationCount":"0","resultStr":"{\"title\":\"Dual-volume reconstruction technology in the detection and classification of recurrent aneurysms following intracranial aneurysm embolization.\",\"authors\":\"Rui Wang, Shuo Leng, Han Xu, Zhiming Tian, Shujuan Xu, Yi Zhang\",\"doi\":\"10.21037/qims-2025-303\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Accurate detection of recurrent intracranial aneurysms (ICAs) after embolization is critical for guiding clinical management and preventing re-rupture. Although two-dimensional digital subtraction angiography (2D-DSA) remains the gold standard, its invasive nature limits routine use. Non-invasive imaging modalities such as computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have limitations in detecting small or morphologically complex recurrent aneurysms. This study aimed to evaluate the diagnostic performance of dual-volume reconstruction technology (DVRT) in comparison to CTA and MRA for detecting recurrent ICA and to explore the correlation between aneurysm imaging characteristics and clinical outcomes.</p><p><strong>Methods: </strong>This retrospective study included 152 patients who underwent ICA embolization and subsequent follow-up imaging with CTA, MRA, and DVRT. All patients received standardized pre-procedural imaging (CTA, MRA, and DVRT) within 48 hours before intervention to document baseline aneurysm characteristics including size, morphology, and location. Postoperative surveillance was systematically performed using triple-modality imaging (CTA, MRA, and DVRT) at 3- and 12-month intervals to monitor treatment efficacy and detect potential recurrence. For the classification of recurrent aneurysms, post-embolization imaging attributes (size, morphology, location) were compared to pre-embolization baseline data to confirm recurrence. Multivariable logistic regression analysis was applied to pre-embolization characteristics to predict recurrence risk. Visualization techniques, including heatmaps and forest plots, were used to illustrate comparative detection performance.</p><p><strong>Results: </strong>DVRT demonstrated higher detection rates for recurrent aneurysms (94.4%, 17/18) compared to CTA (77.8%, 14/18) and MRA (50.0%, 9/18) (P<0.001), with notable performance for small aneurysms (<5 mm: 80.0% <i>vs.</i> 60.0% <i>vs.</i> 40.0%; P=0.317) and medium aneurysms (5-10 mm: 100.0% <i>vs.</i> 88.9% <i>vs.</i> 55.6%; P=0.012). Morphological analysis showed that DVRT had high detection rates for saccular (100.0% <i>vs.</i> 88.9% <i>vs.</i> 66.7%; P=0.039) and lobulated aneurysms (100.0% <i>vs.</i> 75.0% <i>vs.</i> 50.0%; P=0.250), while maintaining detection rates of 92.3% for anterior circulation (<i>vs.</i> 76.9% <i>vs.</i> 46.2%; P=0.008) and 100.0% for posterior circulation aneurysms (<i>vs.</i> 80.0% <i>vs.</i> 60.0%; P=0.200) compared to CTA and MRA, respectively. Multivariable analysis identified size >10 mm [odds ratio (OR) =2.51, 95% confidence interval (CI): 1.83-3.51, P=0.030], irregular morphology (OR =3.02, 95% CI: 2.15-4.43, P=0.003), and posterior location (OR =2.07, 95% CI: 1.43-2.91, P<0.001) as independent predictors of recurrence. Heatmap and forest plot analyses highlighted DVRT's improved diagnostic consistency and narrower CIs across different aneurysm subtypes.</p><p><strong>Conclusions: </strong>DVRT offers superior diagnostic accuracy in detecting recurrent ICA following embolization compared to CTA and MRA, particularly for small, irregularly shaped, and posterior circulation aneurysms. Its advanced imaging capabilities support early detection of recurrence, informed risk stratification, and optimized clinical management strategies. Integration of DVRT into routine postoperative surveillance may improve long-term outcomes for patients with ICA.</p>\",\"PeriodicalId\":54267,\"journal\":{\"name\":\"Quantitative Imaging in Medicine and Surgery\",\"volume\":\"15 9\",\"pages\":\"8008-8022\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397631/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quantitative Imaging in Medicine and Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/qims-2025-303\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-2025-303","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
摘要
背景:颅内动脉瘤栓塞后复发的准确检测对于指导临床处理和预防再破裂至关重要。尽管二维数字减影血管造影(2D-DSA)仍然是金标准,但其侵入性限制了常规使用。非侵入性成像方式,如计算机断层血管造影(CTA)和磁共振血管造影(MRA)在检测小的或形态复杂的复发性动脉瘤方面有局限性。本研究旨在评价双容积重建技术(dual-volume reconstruction technology, DVRT)与CTA、MRA对复发性ICA的诊断价值,探讨动脉瘤影像学特征与临床预后的相关性。方法:本回顾性研究纳入了152例接受ICA栓塞治疗的患者,并进行了CTA、MRA和DVRT随访。所有患者在干预前48小时内接受了标准化的术前成像(CTA, MRA和DVRT),以记录基线动脉瘤特征,包括大小,形态和位置。术后监测采用三模成像(CTA、MRA和DVRT),每隔3个月和12个月进行一次系统监测,以监测治疗效果并检测潜在复发。对于复发动脉瘤的分类,将栓塞后的影像学属性(大小、形态、位置)与栓塞前的基线数据进行比较,以确认复发。多变量logistic回归分析栓塞前特征预测复发风险。可视化技术,包括热图和森林图,用来说明比较检测性能。结果:DVRT对复发动脉瘤的检出率(94.4%,17/18)高于CTA(77.8%, 14/18)和MRA (50.0%, 9/18) (Pvs. 60.0% vs. 40.0%, P=0.317)和中动脉瘤(5-10 mm: 100.0% vs. 88.9% vs. 55.6%, P=0.012)。形态学分析显示,与CTA和MRA相比,DVRT对囊状动脉瘤(100.0% vs. 88.9% vs. 66.7%, P=0.039)和分叶状动脉瘤(100.0% vs. 75.0% vs. 50.0%, P=0.250)的检出率较高,对前循环动脉瘤(76.9% vs. 46.2%, P=0.008)和后循环动脉瘤(80.0% vs. 60.0%, P=0.200)的检出率分别为92.3%和100.0%。多变量分析确定了大小为bbb10 mm[比值比(OR) =2.51, 95%可信区间(CI): 1.83-3.51, P=0.030]、不规则形态(OR =3.02, 95% CI: 2.15-4.43, P=0.003)和后部位置(OR =2.07, 95% CI: 1.43-2.91, P)。结论:与CTA和MRA相比,DVRT在检测栓塞后复发性ICA方面具有更高的诊断准确性,特别是对于小的、不规则形状的和后循环动脉瘤。其先进的成像能力支持早期发现复发,知情的风险分层和优化的临床管理策略。将DVRT纳入术后常规监测可改善ICA患者的长期预后。
Dual-volume reconstruction technology in the detection and classification of recurrent aneurysms following intracranial aneurysm embolization.
Background: Accurate detection of recurrent intracranial aneurysms (ICAs) after embolization is critical for guiding clinical management and preventing re-rupture. Although two-dimensional digital subtraction angiography (2D-DSA) remains the gold standard, its invasive nature limits routine use. Non-invasive imaging modalities such as computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have limitations in detecting small or morphologically complex recurrent aneurysms. This study aimed to evaluate the diagnostic performance of dual-volume reconstruction technology (DVRT) in comparison to CTA and MRA for detecting recurrent ICA and to explore the correlation between aneurysm imaging characteristics and clinical outcomes.
Methods: This retrospective study included 152 patients who underwent ICA embolization and subsequent follow-up imaging with CTA, MRA, and DVRT. All patients received standardized pre-procedural imaging (CTA, MRA, and DVRT) within 48 hours before intervention to document baseline aneurysm characteristics including size, morphology, and location. Postoperative surveillance was systematically performed using triple-modality imaging (CTA, MRA, and DVRT) at 3- and 12-month intervals to monitor treatment efficacy and detect potential recurrence. For the classification of recurrent aneurysms, post-embolization imaging attributes (size, morphology, location) were compared to pre-embolization baseline data to confirm recurrence. Multivariable logistic regression analysis was applied to pre-embolization characteristics to predict recurrence risk. Visualization techniques, including heatmaps and forest plots, were used to illustrate comparative detection performance.
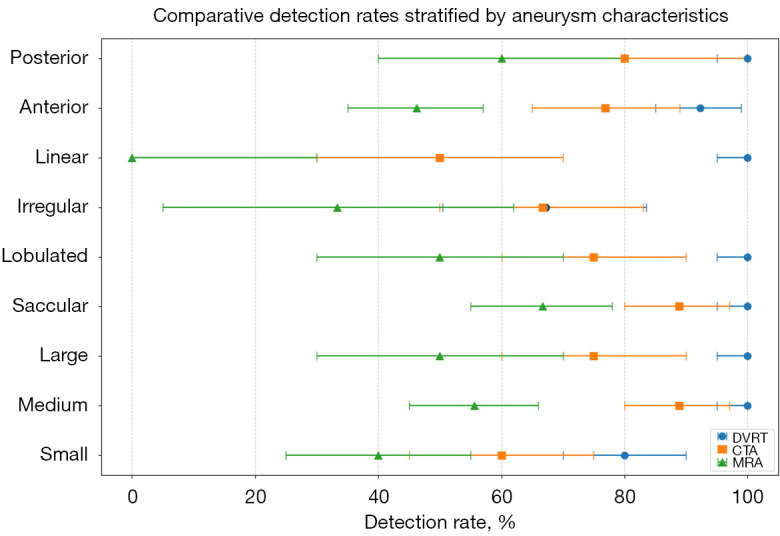
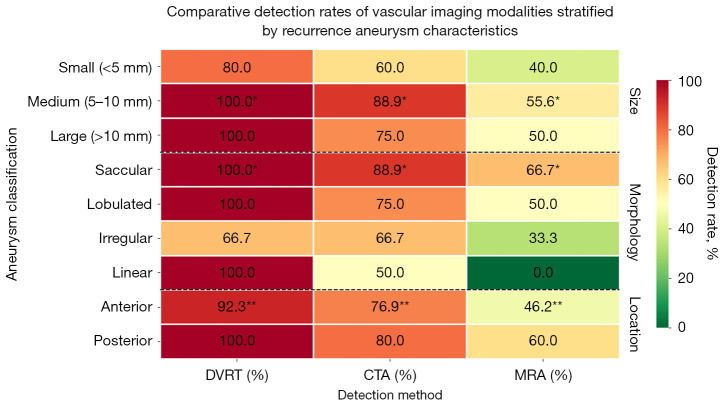
Results: DVRT demonstrated higher detection rates for recurrent aneurysms (94.4%, 17/18) compared to CTA (77.8%, 14/18) and MRA (50.0%, 9/18) (P<0.001), with notable performance for small aneurysms (<5 mm: 80.0% vs. 60.0% vs. 40.0%; P=0.317) and medium aneurysms (5-10 mm: 100.0% vs. 88.9% vs. 55.6%; P=0.012). Morphological analysis showed that DVRT had high detection rates for saccular (100.0% vs. 88.9% vs. 66.7%; P=0.039) and lobulated aneurysms (100.0% vs. 75.0% vs. 50.0%; P=0.250), while maintaining detection rates of 92.3% for anterior circulation (vs. 76.9% vs. 46.2%; P=0.008) and 100.0% for posterior circulation aneurysms (vs. 80.0% vs. 60.0%; P=0.200) compared to CTA and MRA, respectively. Multivariable analysis identified size >10 mm [odds ratio (OR) =2.51, 95% confidence interval (CI): 1.83-3.51, P=0.030], irregular morphology (OR =3.02, 95% CI: 2.15-4.43, P=0.003), and posterior location (OR =2.07, 95% CI: 1.43-2.91, P<0.001) as independent predictors of recurrence. Heatmap and forest plot analyses highlighted DVRT's improved diagnostic consistency and narrower CIs across different aneurysm subtypes.
Conclusions: DVRT offers superior diagnostic accuracy in detecting recurrent ICA following embolization compared to CTA and MRA, particularly for small, irregularly shaped, and posterior circulation aneurysms. Its advanced imaging capabilities support early detection of recurrence, informed risk stratification, and optimized clinical management strategies. Integration of DVRT into routine postoperative surveillance may improve long-term outcomes for patients with ICA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


