{"title":"冠状动脉钙评分与心血管事件的关联:一项回顾性研究。","authors":"Xun Yu, Guifang Li, Wenbo Yin, Junni Hu","doi":"10.21037/qims-2025-549","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The coronary artery calcium score (CACS) reflects coronary atherosclerosis burden, but its predictive value in different populations remains to be fully elucidated. The aim of this study was to investigate the predictive value of CACS for cardiovascular events in different patient populations.</p><p><strong>Methods: </strong>One hundred patients (mean age 65.4±10.7 years; 63 males) who underwent coronary computed tomography angiography (CCTA) were retrospectively enrolled and classified into four CACS strata (0, 1-100, 101-399, ≥400). The primary endpoint was all-cause mortality and major adverse cardiovascular events (MACEs) at 1 year. Survival curves and Cox regression were performed.</p><p><strong>Results: </strong>Patients with CACS ≥400 had the lowest 1-year survival probability (log-rank P=0.011), while CACS =0 group had the highest survival. Cox regression suggested CACS ≥400 was associated with a 4.76-fold higher risk of mortality or MACE compared to CACS =0 [adjusted hazard ratio (HR) 4.76, 95% confidence interval (CI): 1.82-12.45, P=0.012], after adjusting for age, sex, hypertension, diabetes, and dyslipidemia. Significant predictors included male sex (HR 3.72, P=0.047), smoking (HR 2.87, P=0.013), and hypertension (HR 4.76, P=0.009). In subgroup analysis, the predictive value of CACS was robust in males (P=0.0031) and hypertensive patients (P=0.021), but not significant in females or normotensives (P>0.5).</p><p><strong>Conclusions: </strong>CACS is a significant independent predictor of mortality and MACE in symptomatic patients, with the strongest discriminative power in males and those with hypertension. These findings support the utility of CACS for risk stratification and early identification of high-risk individuals in clinical practice.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8230-8238"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397672/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association of coronary artery calcium score with cardiovascular events: a retrospective study.\",\"authors\":\"Xun Yu, Guifang Li, Wenbo Yin, Junni Hu\",\"doi\":\"10.21037/qims-2025-549\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The coronary artery calcium score (CACS) reflects coronary atherosclerosis burden, but its predictive value in different populations remains to be fully elucidated. The aim of this study was to investigate the predictive value of CACS for cardiovascular events in different patient populations.</p><p><strong>Methods: </strong>One hundred patients (mean age 65.4±10.7 years; 63 males) who underwent coronary computed tomography angiography (CCTA) were retrospectively enrolled and classified into four CACS strata (0, 1-100, 101-399, ≥400). The primary endpoint was all-cause mortality and major adverse cardiovascular events (MACEs) at 1 year. Survival curves and Cox regression were performed.</p><p><strong>Results: </strong>Patients with CACS ≥400 had the lowest 1-year survival probability (log-rank P=0.011), while CACS =0 group had the highest survival. Cox regression suggested CACS ≥400 was associated with a 4.76-fold higher risk of mortality or MACE compared to CACS =0 [adjusted hazard ratio (HR) 4.76, 95% confidence interval (CI): 1.82-12.45, P=0.012], after adjusting for age, sex, hypertension, diabetes, and dyslipidemia. Significant predictors included male sex (HR 3.72, P=0.047), smoking (HR 2.87, P=0.013), and hypertension (HR 4.76, P=0.009). In subgroup analysis, the predictive value of CACS was robust in males (P=0.0031) and hypertensive patients (P=0.021), but not significant in females or normotensives (P>0.5).</p><p><strong>Conclusions: </strong>CACS is a significant independent predictor of mortality and MACE in symptomatic patients, with the strongest discriminative power in males and those with hypertension. These findings support the utility of CACS for risk stratification and early identification of high-risk individuals in clinical practice.</p>\",\"PeriodicalId\":54267,\"journal\":{\"name\":\"Quantitative Imaging in Medicine and Surgery\",\"volume\":\"15 9\",\"pages\":\"8230-8238\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397672/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quantitative Imaging in Medicine and Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/qims-2025-549\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-2025-549","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Association of coronary artery calcium score with cardiovascular events: a retrospective study.
Background: The coronary artery calcium score (CACS) reflects coronary atherosclerosis burden, but its predictive value in different populations remains to be fully elucidated. The aim of this study was to investigate the predictive value of CACS for cardiovascular events in different patient populations.
Methods: One hundred patients (mean age 65.4±10.7 years; 63 males) who underwent coronary computed tomography angiography (CCTA) were retrospectively enrolled and classified into four CACS strata (0, 1-100, 101-399, ≥400). The primary endpoint was all-cause mortality and major adverse cardiovascular events (MACEs) at 1 year. Survival curves and Cox regression were performed.
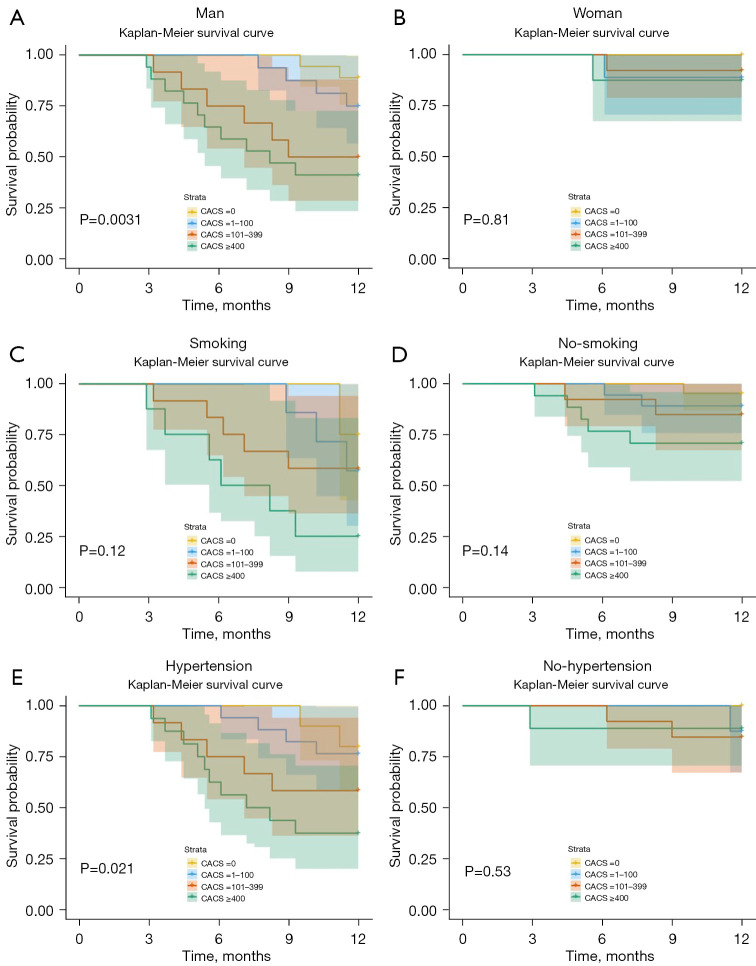
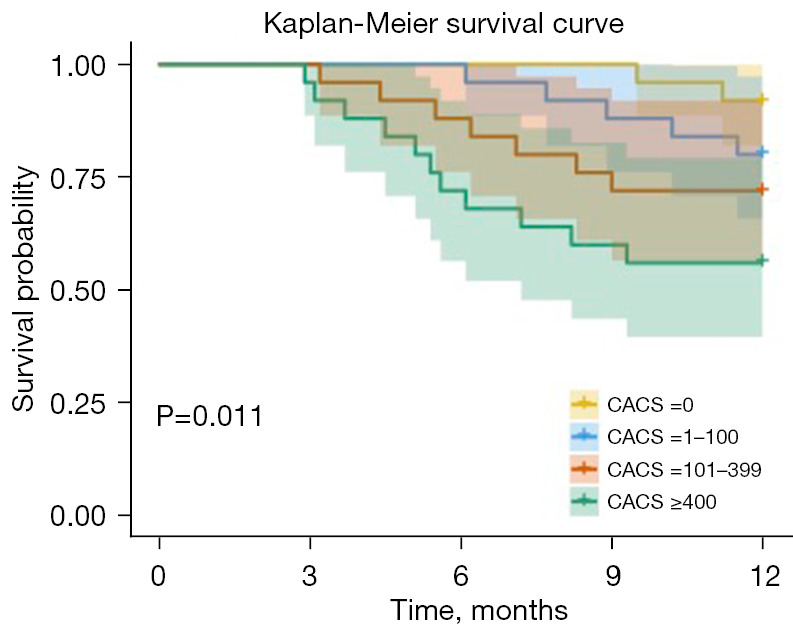
Results: Patients with CACS ≥400 had the lowest 1-year survival probability (log-rank P=0.011), while CACS =0 group had the highest survival. Cox regression suggested CACS ≥400 was associated with a 4.76-fold higher risk of mortality or MACE compared to CACS =0 [adjusted hazard ratio (HR) 4.76, 95% confidence interval (CI): 1.82-12.45, P=0.012], after adjusting for age, sex, hypertension, diabetes, and dyslipidemia. Significant predictors included male sex (HR 3.72, P=0.047), smoking (HR 2.87, P=0.013), and hypertension (HR 4.76, P=0.009). In subgroup analysis, the predictive value of CACS was robust in males (P=0.0031) and hypertensive patients (P=0.021), but not significant in females or normotensives (P>0.5).
Conclusions: CACS is a significant independent predictor of mortality and MACE in symptomatic patients, with the strongest discriminative power in males and those with hypertension. These findings support the utility of CACS for risk stratification and early identification of high-risk individuals in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


